Image


▼This medicine is subject to additional monitoring. This will allow quick identification of new safety information. Adverse events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov.uk for the UK and hpra.ie/homepage/about-us/report-an-issue for Republic of Ireland. Adverse events should also be reported to UCB Pharma Ltd at ucbcares.uk@ucb.com or 0800 2793177 for the UK and UCB (Pharma) Ireland Ltd at ucbcares.ie@ucb.com or 1800 930075 for Republic of Ireland.
BIMZELX® (bimekizumab) is indicated for the treatment of: active PsA, alone or in combination with methotrexate, in adults who have had an inadequate response or who have been intolerant to one or more DMARDs; active nr-axSpA, in adults with objective signs of inflammation as indicated by elevated CRP and/or MRI, who have responded inadequately or are intolerant to NSAIDs; and active AS, in adults who have responded inadequately or are intolerant to conventional therapy.4

Explore more in ‘Symptom improvement’ section below |
Explore more in ‘Reductions in disease activity’ section below |

Explore more in ‘Inhibition of disease progression’ section below |
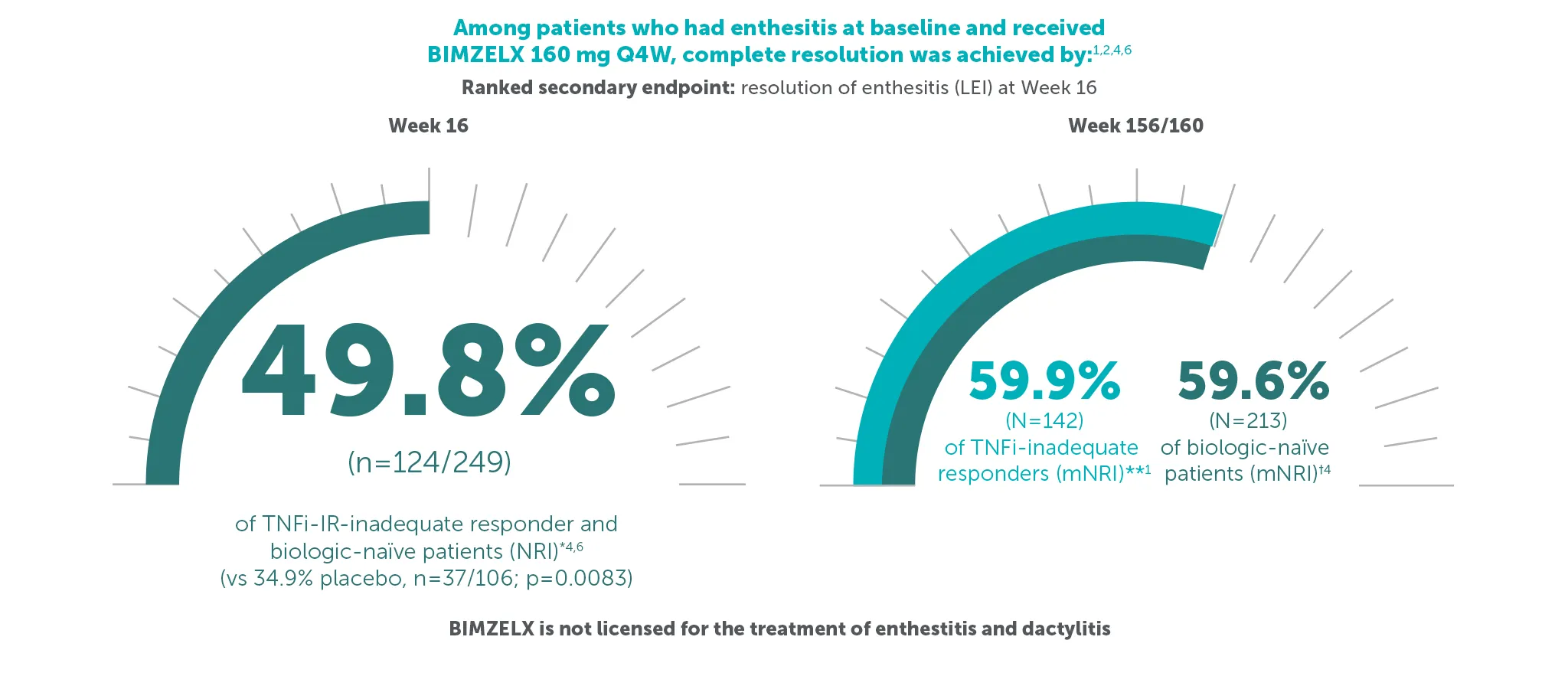
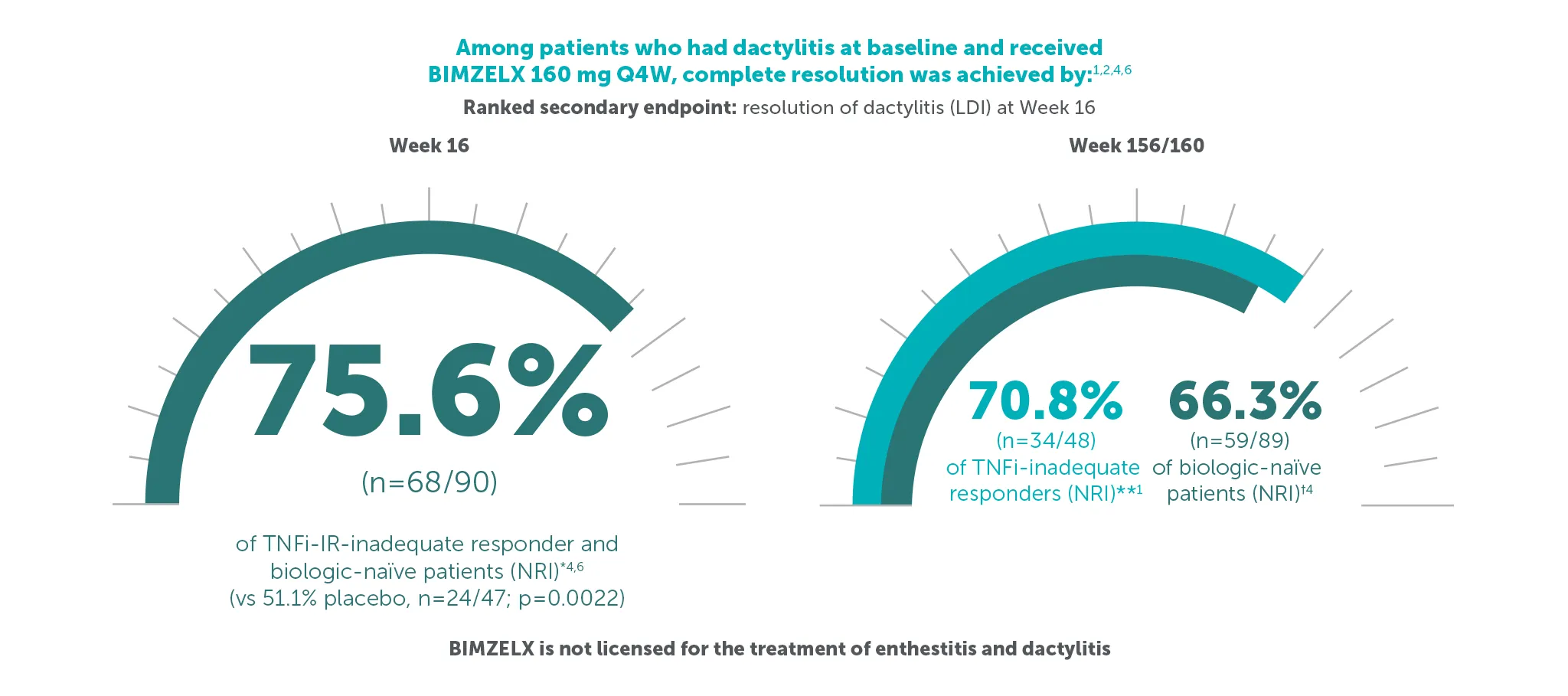
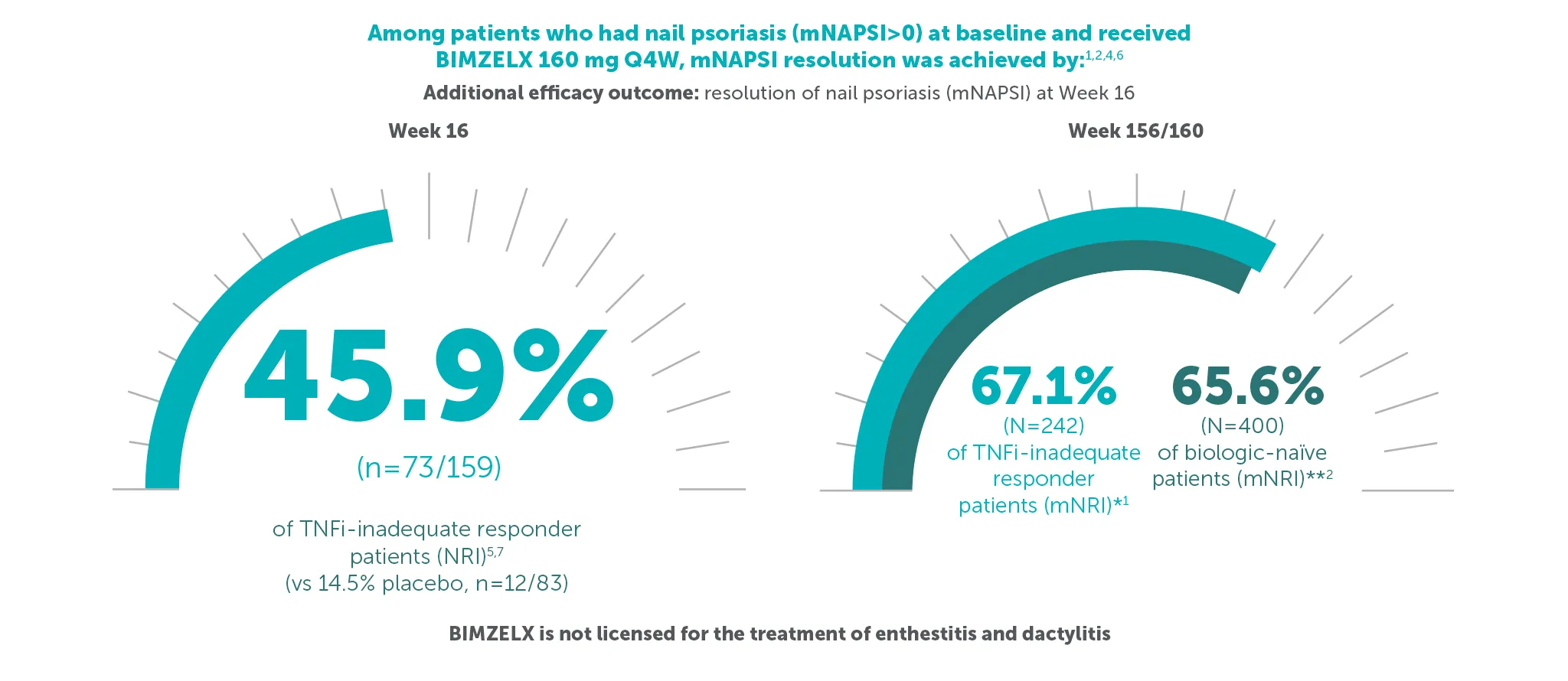
Explore more in ‘Resolution of key manifestations’ section below |
Explore more in ‘Resolution of peripheral arthritis’ section below |
Explore more in ‘Patient-reported outcomes’ section below |
*ACR 50 achieved by 43.4% (116/267) TNFI-IR and 43.9% (189/431) biologic-naïve patients with PsA at Week 16 (primary endpoint in BE COMPLETE and BE OPTIMAL; vs 6.8% (9/133) and 10.0% (28/281) with placebo, respectively; p<0.001), 4–6 51.7% (138/267) and 54.5% (235/431) at Week 52, respectively (NRI analysis).7,8 ACR 50 was achieved by 54.2% (n=400) of TNFI-IR patients at Week 100 and 55.0% (n=712) of biologic-naïve patients at Week 104; 55.2% (n=400) at Week 156 and 53.2% (n=712) at Week 160, respectively, in the BE VITAL OLE in the BIMZELX treatment arms (mNRI analysis).1,2
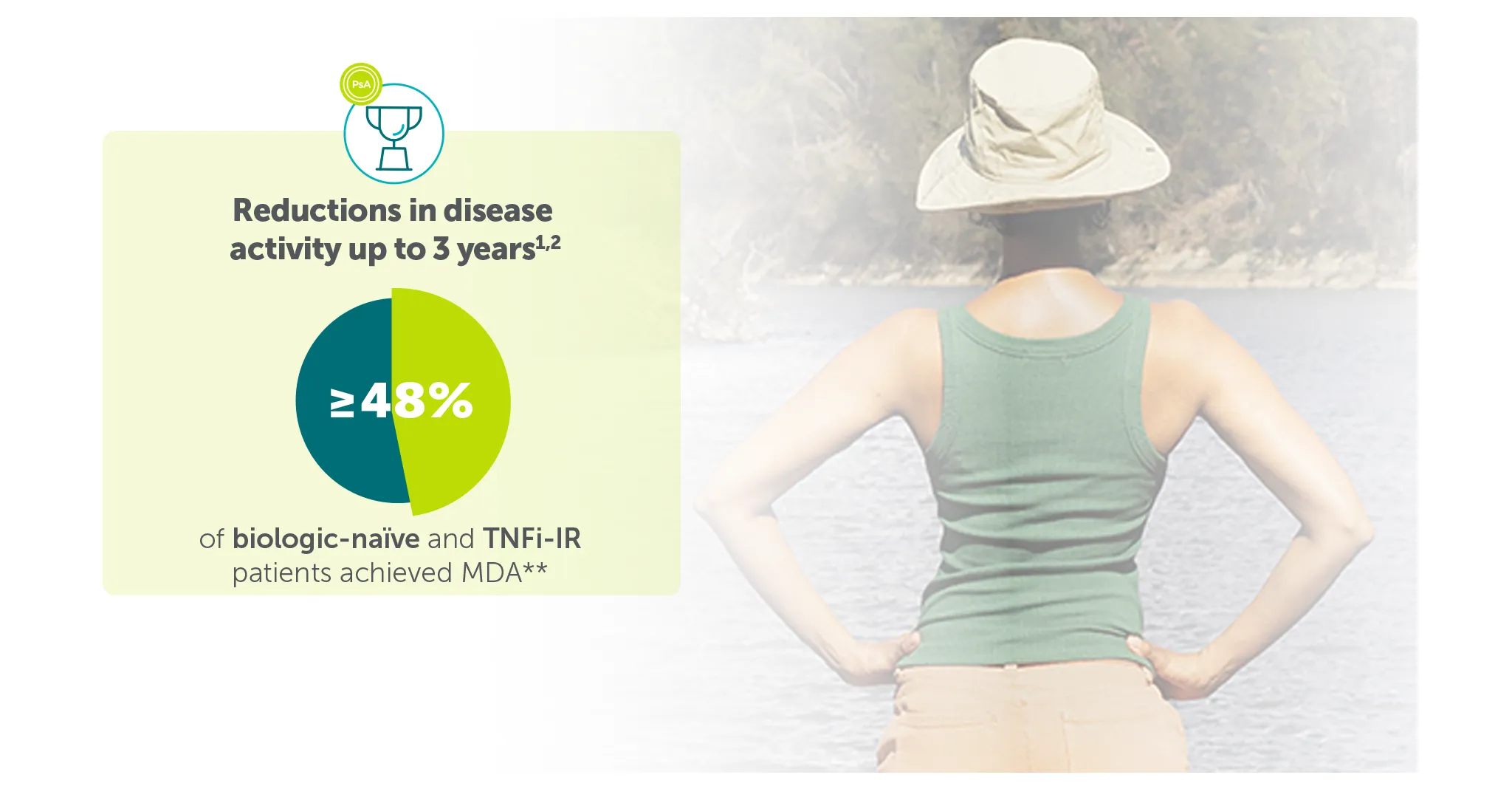
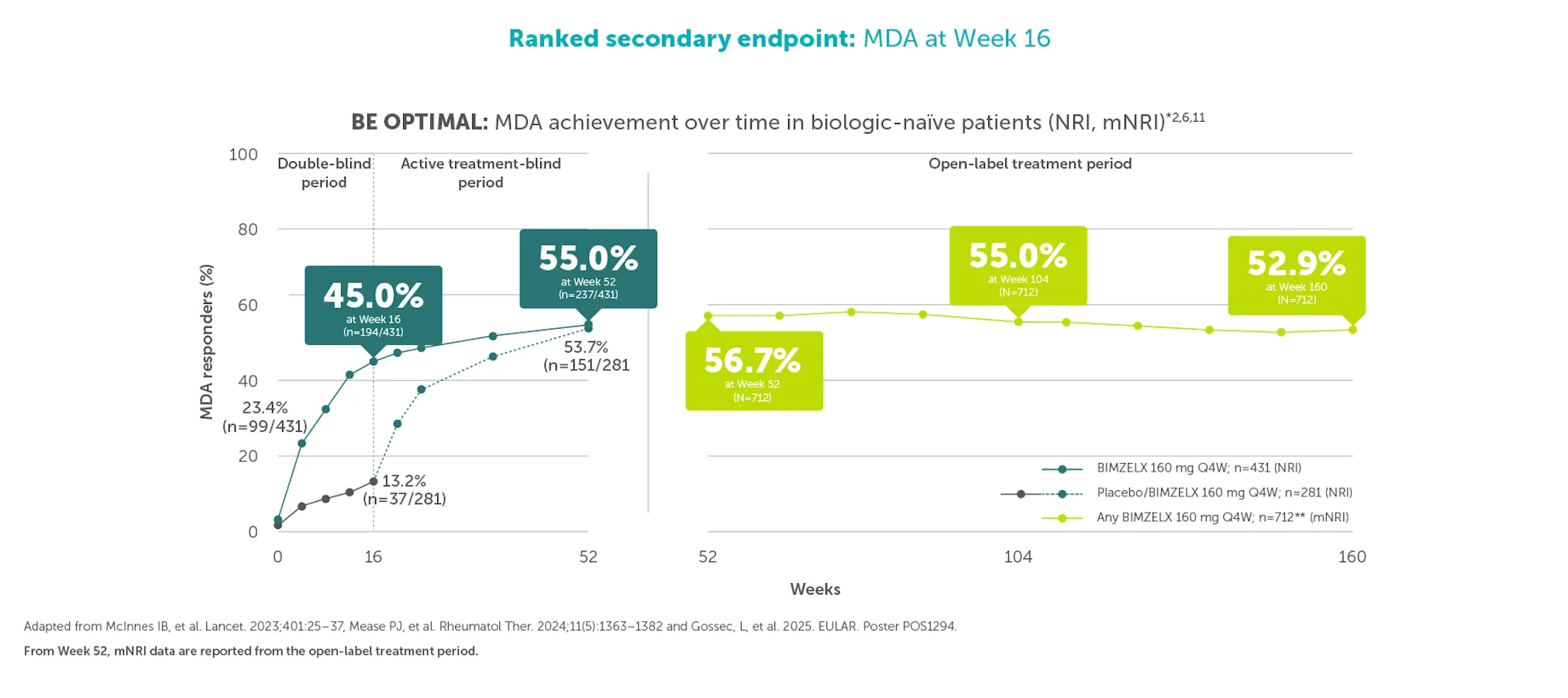
**In BE COMPLETE and the BE VITAL OLE, MDA was achieved by 44.2% (118/267) of TNFI-IR patients in the BIMZELX treatment arm at Week 16 (ranked secondary endpoint; NRI analysis).5 In the open-label treatment period, MDA was achieved by 43.9% of TNFI-IR BIMZELX-treated patients at Week 52, 48.6% at Week 100 and 48.8% at Week 156, respectively (mNRI analysis; n=400).1 In BE OPTIMAL and the BE VITAL OLE, MDA was achieved by 45.0% (194/431) of biologic-naïve patients in the BIMZELX treatment arm at Week 16 (ranked secondary endpoint; NRI analysis).6 In the open-label treatment period, MDA was achieved by 56.7% of biologic-naïve BIMZELX-treated patients at Week 52, 55.0% at Week 104 and 52.9% at Week 160 (mNRI analysis; n=712).2
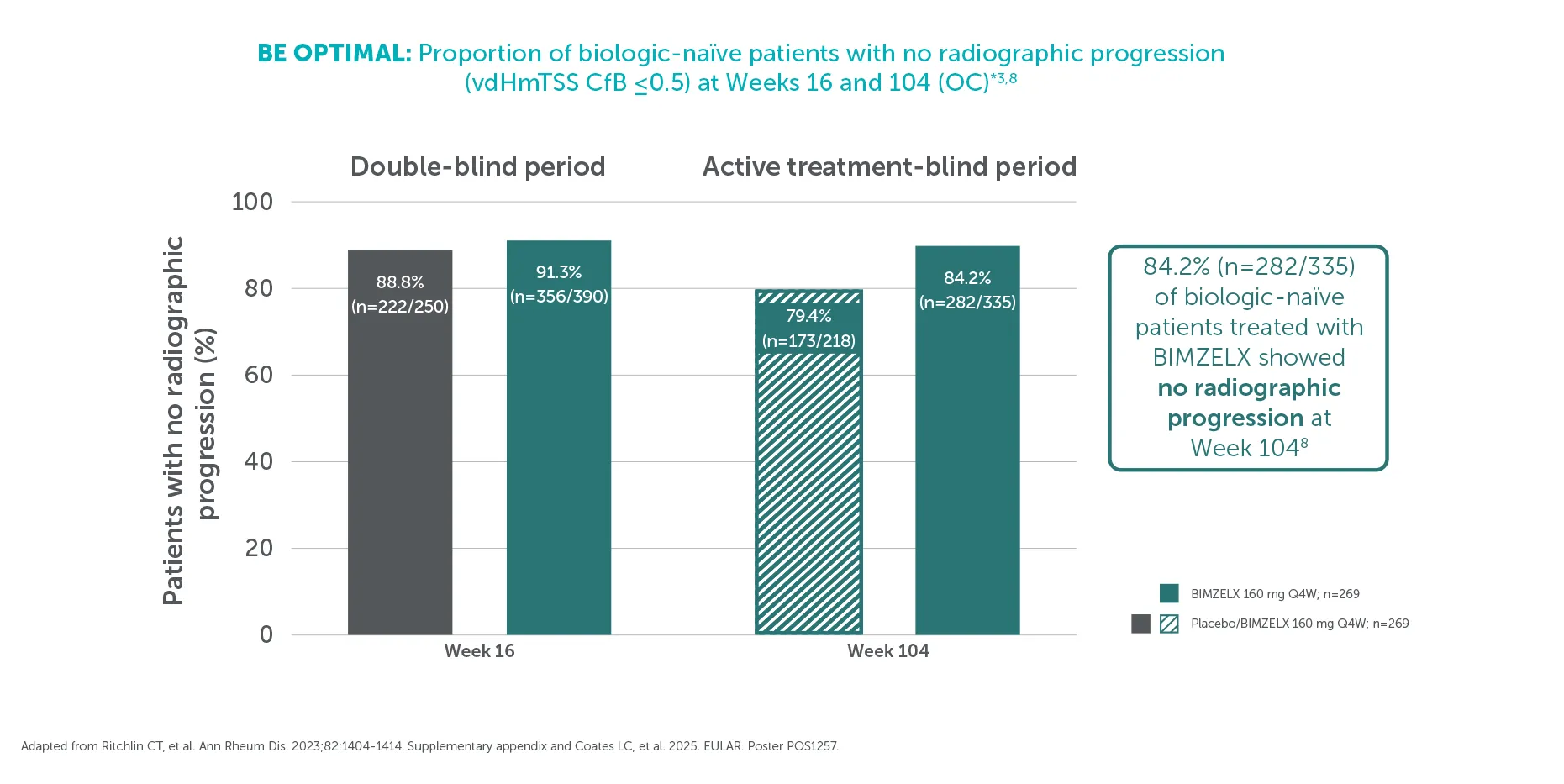
†At Week 104, 84.2% (282/335) of biologic-naïve patients in BE OPTIMAL showed no structural damage progression (defined as vdHmTSS change from baseline ≤0.5) with BIMZELX vs 79.4% (173/218) in the group that switched from placebo to BIMZELX at Week 16 (OC analysis).3
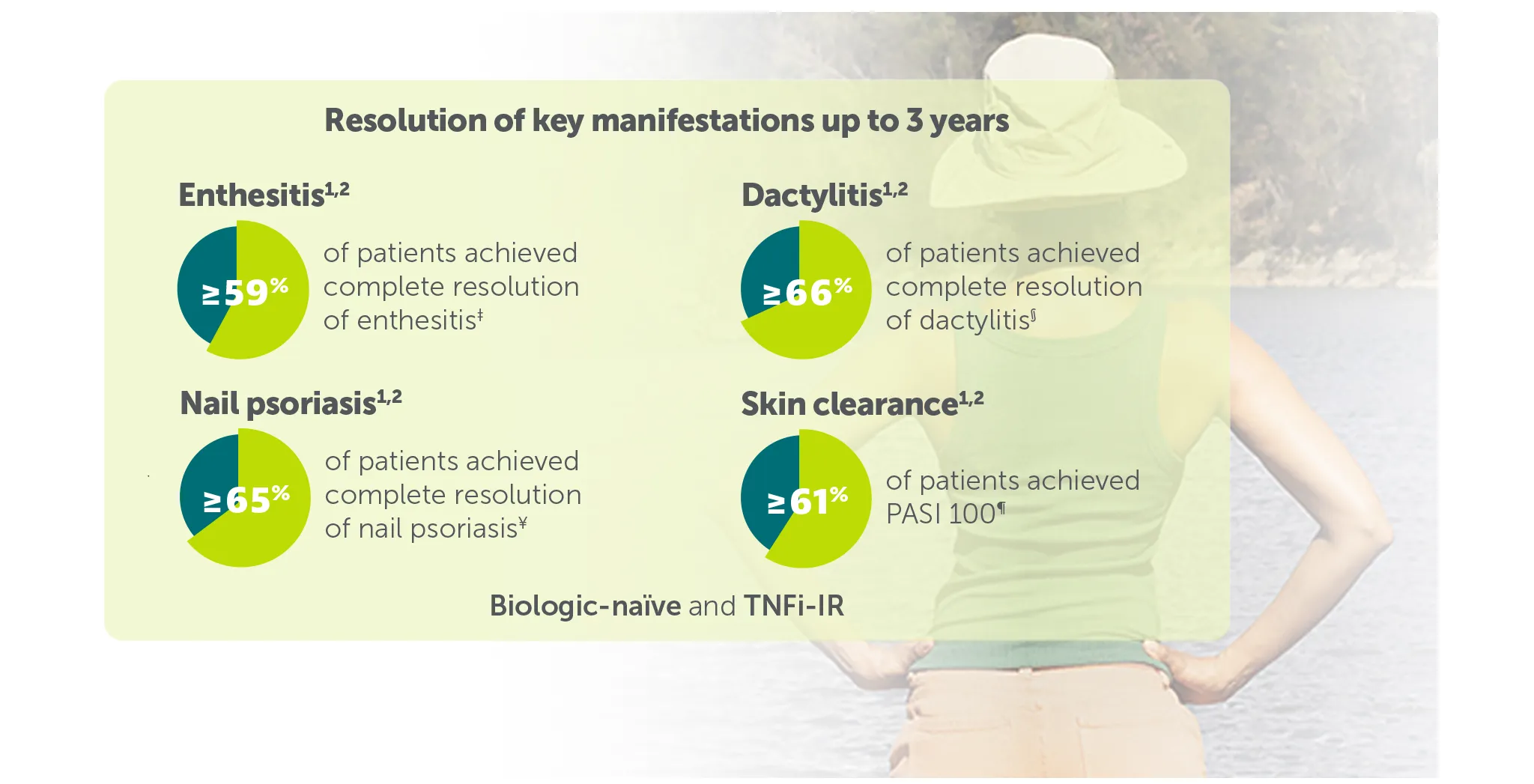
‡59.9% (n=142) of TNFI-IR patients and 59.6% (n=213) of biologic-naïve patients in the BE VITAL OLE of BE COMPLETE and BE OPTIMAL achieved complete resolution of enthesitis (LEI=0) at Weeks 156/160, respectively (additional efficacy outcome in BE COMPLETE and ranked secondary endpoint at Week 16 in BE OPTIMAL, mNRI analysis).1,2,6,7
§70.8% (n=48) of TNFI-IR patients and 66.3% (n=89) of biologic-naïve patients in the BE VITAL OLE of BE COMPLETE and BE OPTIMAL achieved complete resolution of dactylitis (LDI=0) at Weeks 156/160, respectively (additional efficacy outcome in BE COMPLETE and ranked secondary endpoint at Week 16 in BE OPTIMAL, NRI analysis). 1,2,6,7
¥67.1% (n=242) of TNFI-IR patients and 65.6% (n=400) of biologic-naïve patients in the BE VITAL OLE of BE COMPLETE and BE OPTIMAL achieved complete resolution of nail psoriasis (mNAPSI=0) at Weeks 156/160, respectively (additional efficacy outcome in BE COMPLETE and additional efficacy variable at Week 16 in BE OPTIMAL, mNRI analysis).1,2,6,7
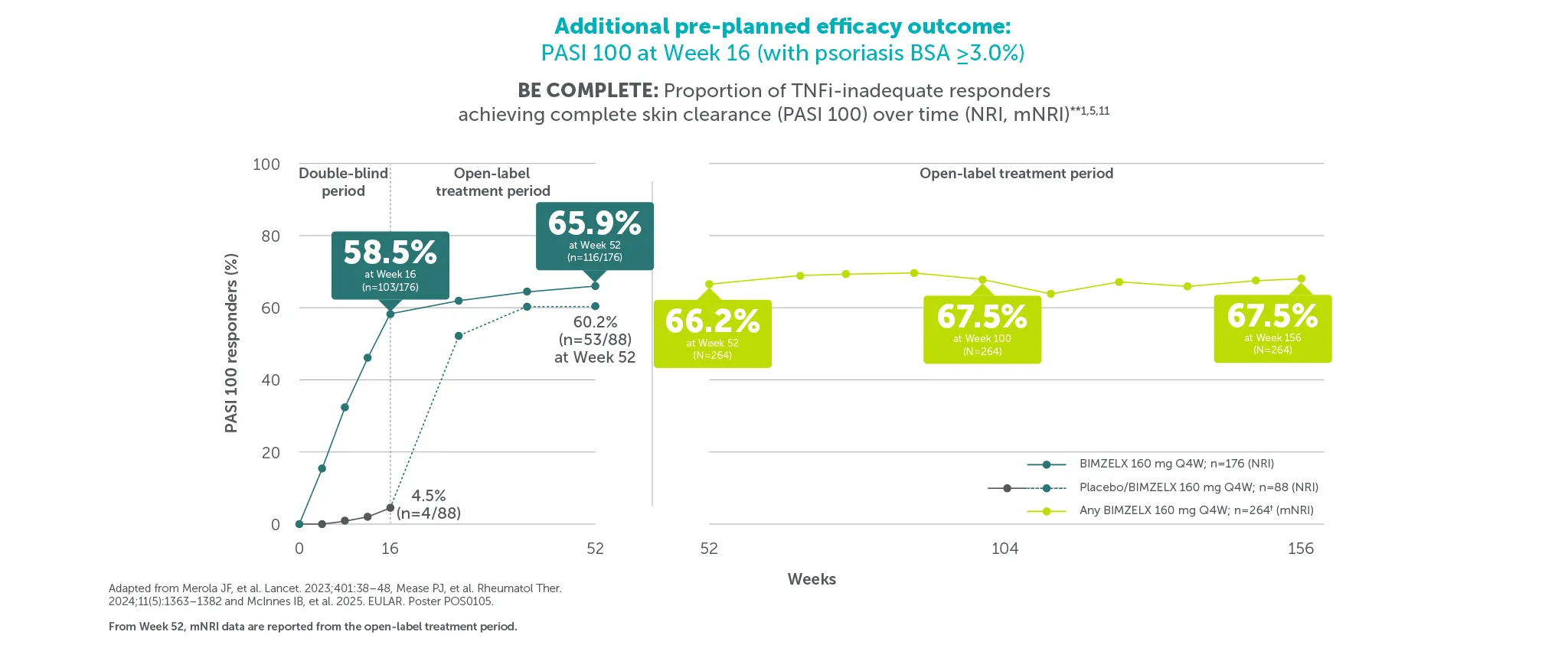
¶58.5% (103/176) and 47.5% (103/217) of patients achieved PASI 100 at Week 16 (vs 4.5% (4/88) and 2.1% (3/140) with placebo) in BE COMPLETE and BE OPTIMAL, respectively (additional pre-planned efficacy outcome at Week 16, NRI analysis).5,6 67.5% (n=264) of TNFI-IR patients and 61.9% (n=357) of biologic-naïve BIMZELX-treated patients achieved PASI 100 at Week 156/160 in the BE VITAL OLE (mNRI analysis).1,2 PASI response in patients with psoriasis involving at least 3% BSA at baseline.1,2
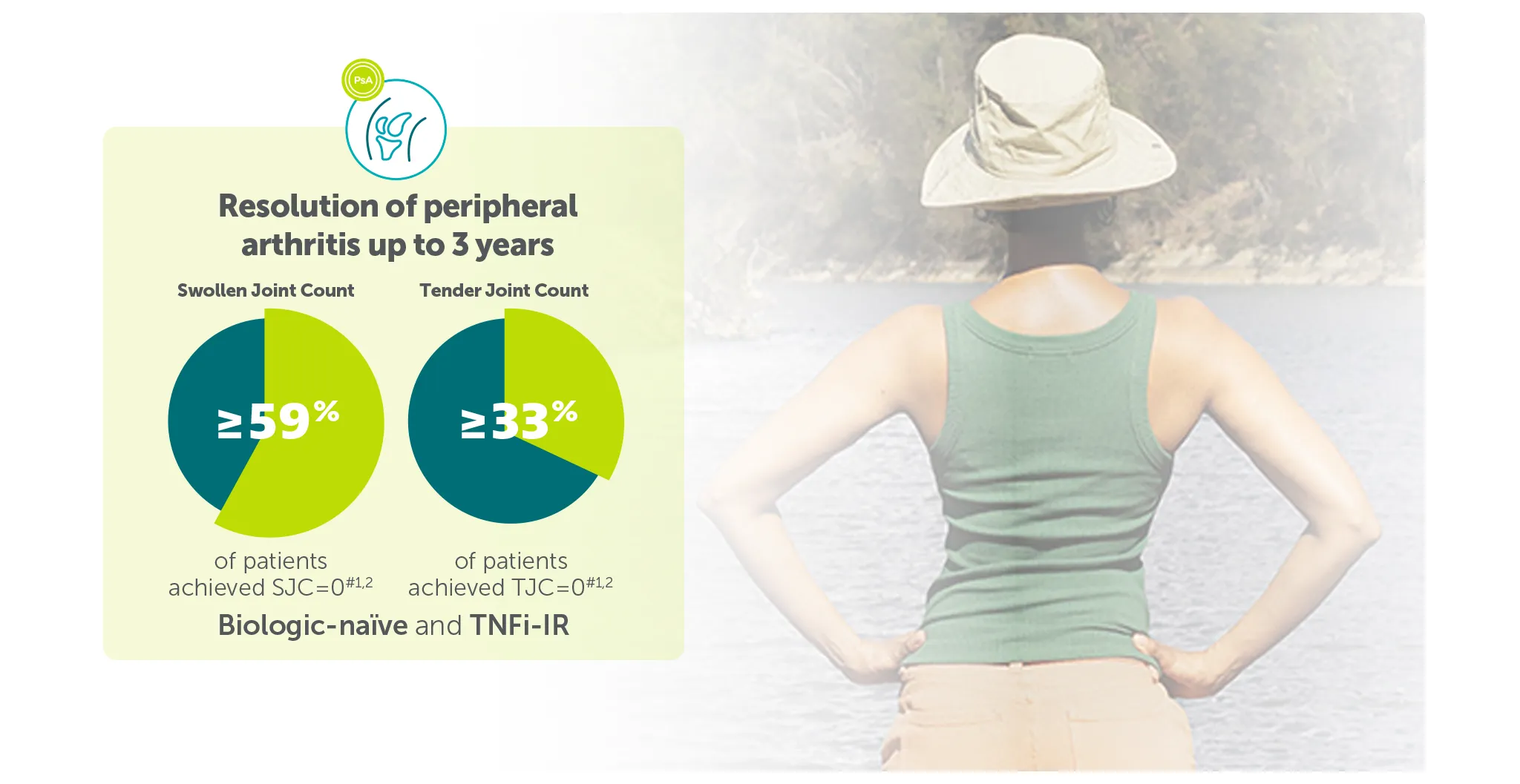
#In the BE VITAL OLE of BE COMPLETE and BE OPTIMAL, SJC=0 was achieved by 59.1% (n=400) of TNFi-IR patients at Week 156 and 59.5% (n=712) of biologic-naïve patients at Week 160 in the BIMZELX treatment arms, respectively (mNRI analysis).1,2 TJC=0 was achieved by 33.0% (n=400) of TNFI-IR patients at Week 156 and 36.9% (n=712) of biologic-naïve patients at Week 160 in the BIMZELX treatment arms, respectively (mNRI).1,2
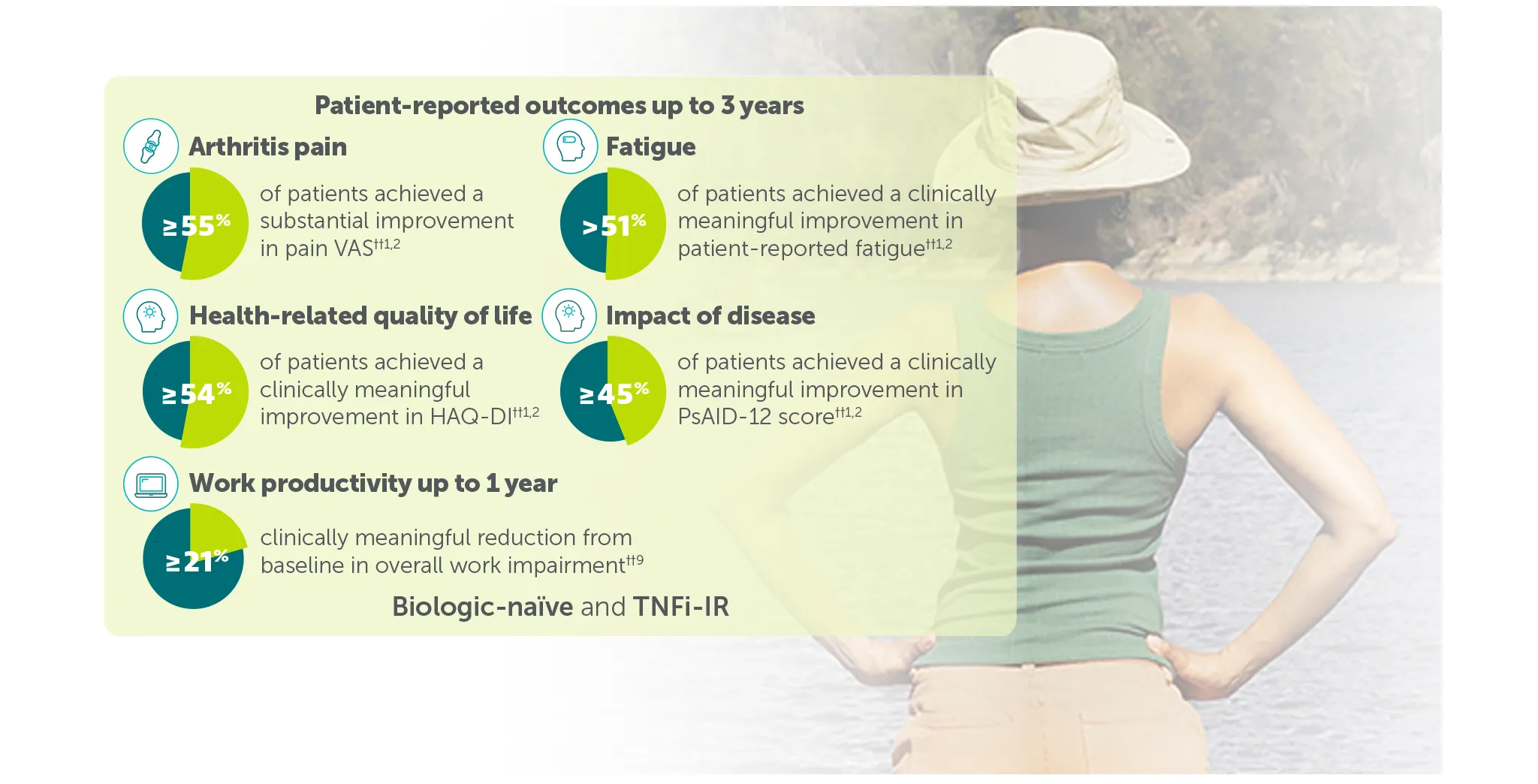
†† In BE VITAL OLE of BE COMPLETE and BE OPTIMAL:
≥50% (substantial) improvement in Pain VAS was achieved by 59.4% (n=400) of TNFI-IR patients and 55.2% (n=712) of biologic-naïve patients at Weeks 156 and 160, respectively (mNRI analysis).1,2
Clinically meaningful improvement in fatigue (FACIT-Fatigue MCID) was achieved by 54.2% (n=371) of TNFI-IR patients and 51.5% (n=643) of biologic-naïve patients at Weeks 156 and 148, respectively (mNRI analysis).1,2 FACIT-Fatigue MCID defined as score increase from baseline ≥4 in patients with FACIT-Fatigue ≤48 at baseline.1,2
Clinically meaningful improvement in HAQ-DI (HAQ-DI MCID) was achieved by 55.7% (n=341) of TNFI-IR patients and 54.4% (n=539) of biologic-naïve patients at Weeks 156 and 160, respectively (mNRI analysis).1,2 HAQ-DI MCID defined as decrease from baseline ≥0.35 in patients with HAQ-DI ≥0.35 at baseline).1,2
50.8% (n=299) of TNFI-IR patients and 45.6% (n=494) of biologic-naïve patients in the BIMZELX treatment arms achieved clinically meaningful reductions in disease impact at Weeks 156 and 148, respectively (mNRI analysis).1,2 Clinically meaningful improvement response: ≥3-point decrease from baseline when respective PsAID-12 score was >3 at baseline.1,2
In TNFI-IR patients, mean percentage reduction from baseline in overall work impairment was 21.5% (n=128) at Week 40 in the BIMZELX treatment arm (OC analysis).9 In biologic-naïve patients, mean percentage reduction from baseline in overall work impairment was 21.3% (n=206) at Week 52 in the BIMZELX treatment arm (OC analysis).9 Clinically meaningful improvement in overall work impairment was estimated to be 15%.9,10
From Week 52, mNRI data are reported from the open-label treatment period.
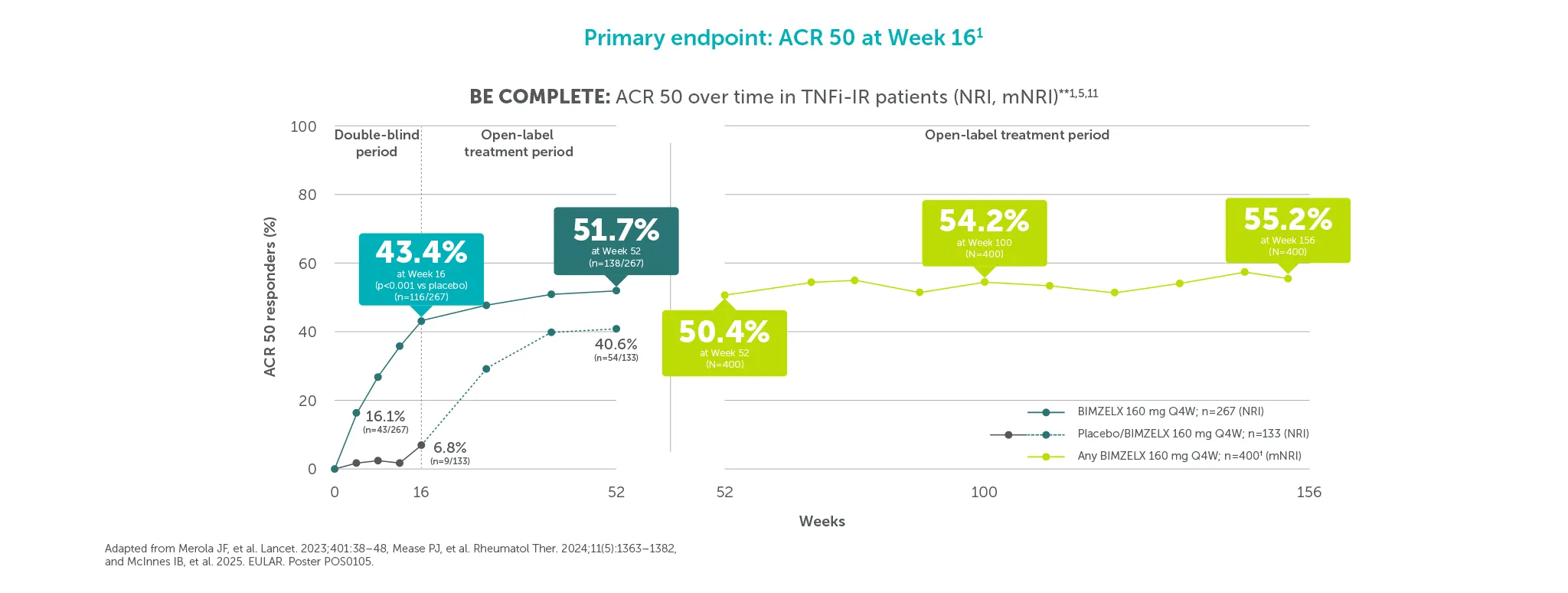
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase 3 trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study. In BE COMPLETE, after Week 16, the investigators and subjects remained blind to the assigned BIMZELX dosing regimen until the final analysis was completed.5
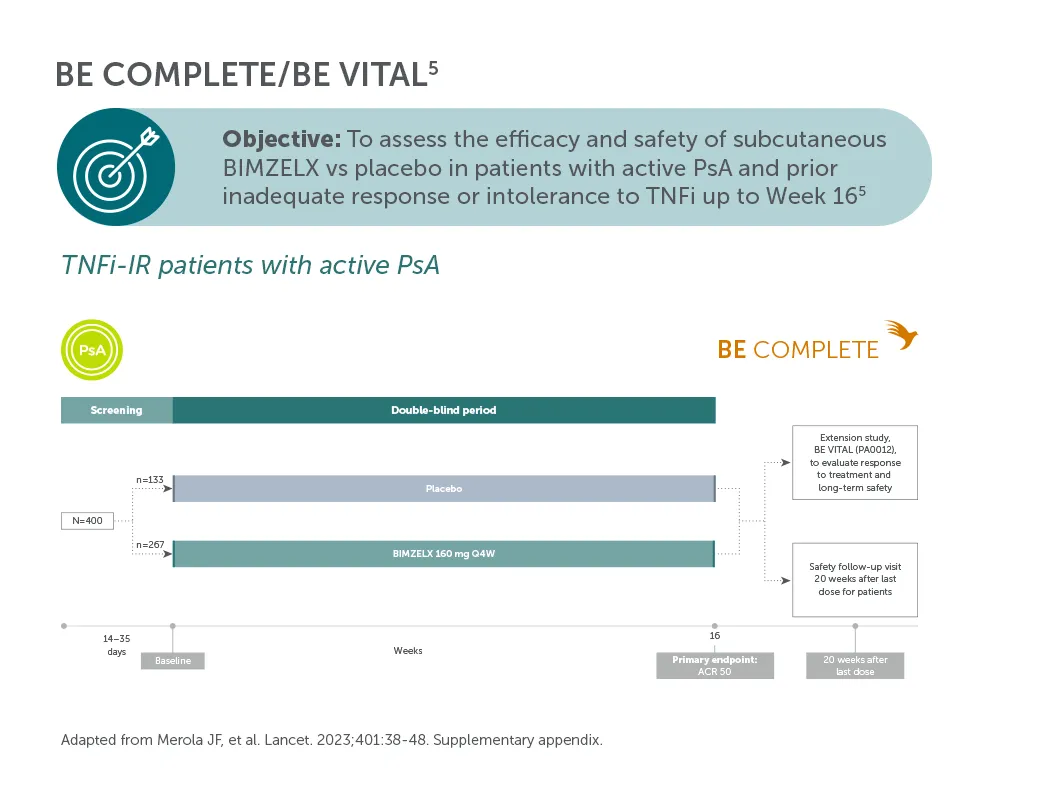
*In BE COMPLETE, ACR 50 was achieved by 16.1% (43/267) of BIMZELX-treated TNF-IR patients with PsA at Week 4.5 43.4% (116/267) at Week 16 (primary endpoint; p<0.001 vs placebo),4,5 and 51.7% (138/267) at Week 52 (NRI analysis).7 In the open-label treatment period, ACR 50 was achieved by 50.4% of BIMZELX-treated TNFI-IR patients with PsA at Week 52, 54.2% at Week 100, and 55.2% at Week 156 (mNRI analysis; N=400).1 Some n values are unavailable due to the imputation method used. **Of patients who entered the OLE at Week 16, 74.8% (299/400) remained on treatment at Week 156.1 †Includes patients originally randomised to placebo.1,5,11
From Week 52, mNRI data are reported from the open-label treatment period.
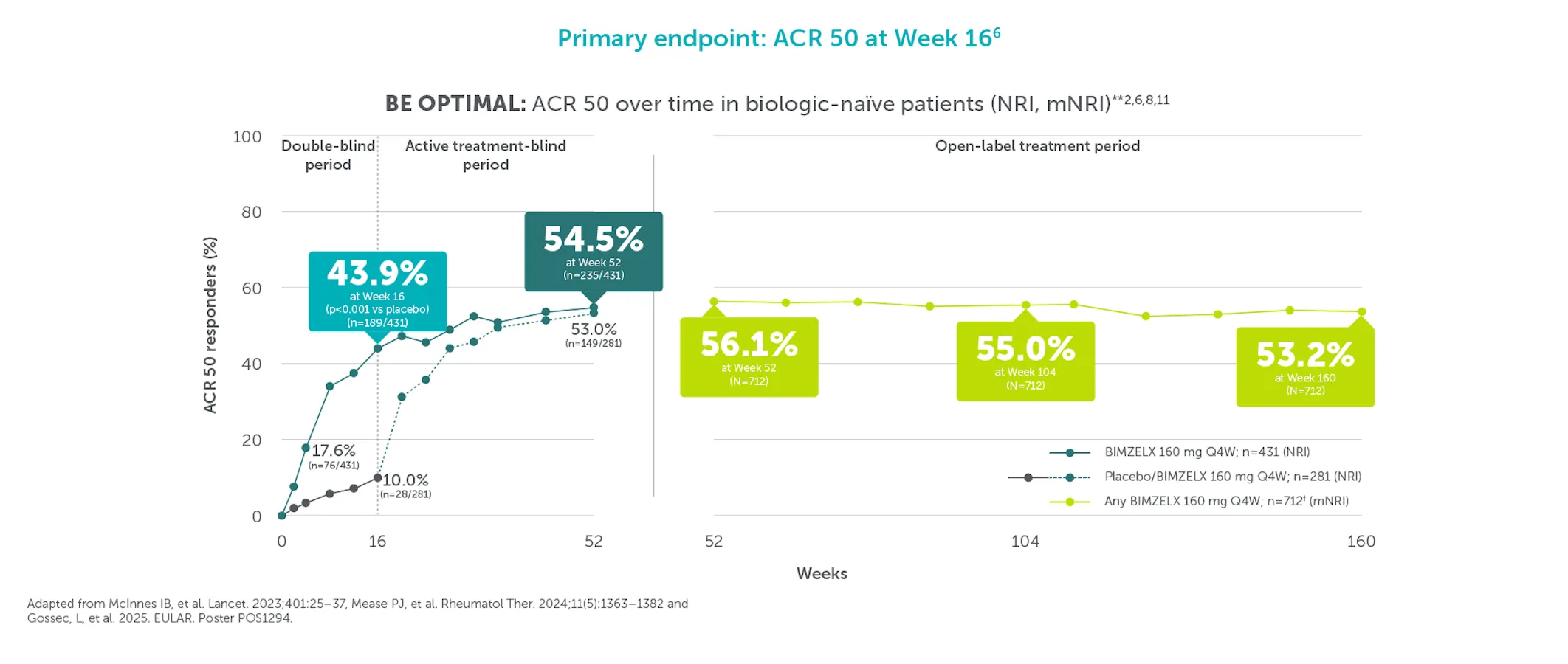
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results.
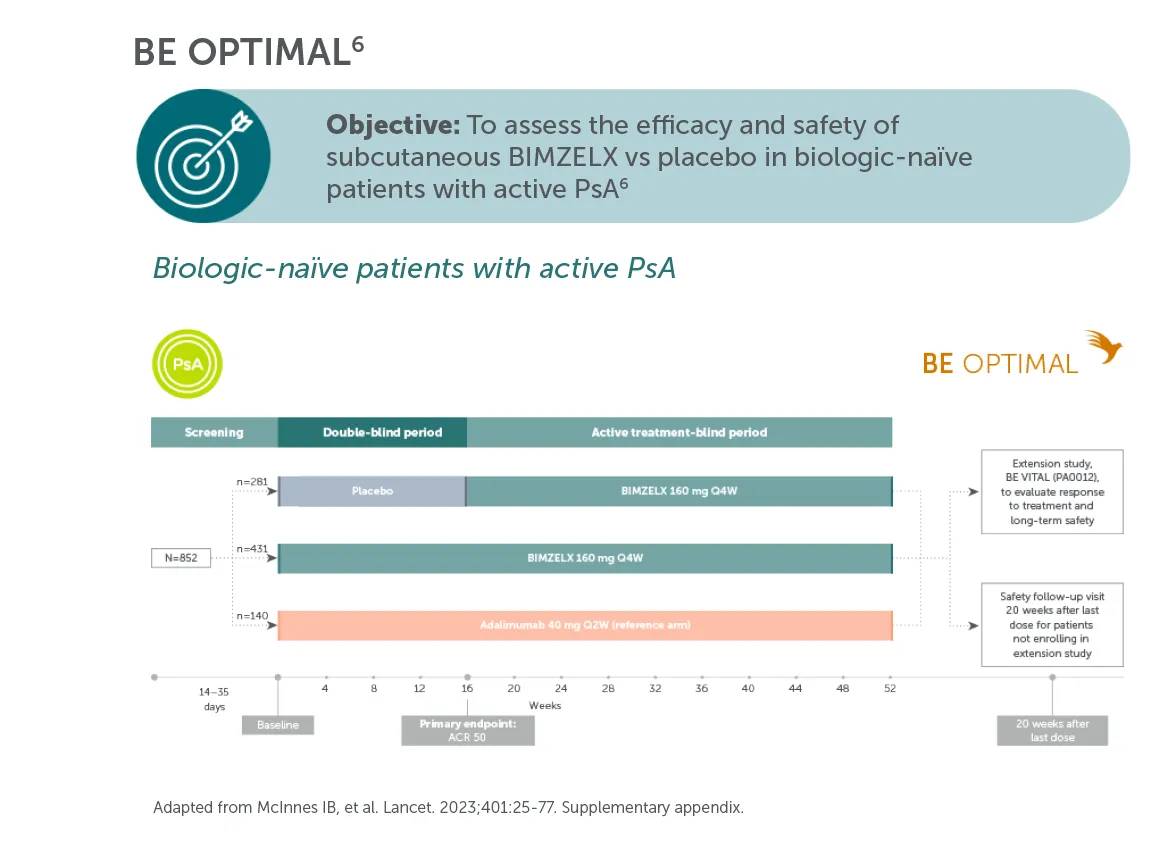
*In BE OPTIMAL, ACR 50 was achieved by 17.6% (076/431) of BIMZELX-treated biologic-naïve patients with PsA at Week 4, 43.9% (189/431) at Week 16 (primary endpoint, p<0.001 vs placebo),4,6,8 and 54.5% (235/431) at Week 52 (NRI analysis).8 In the open-label treatment period, ACR 50 was achieved by 56.1% of BIMZELX-treated biologic-naïve patients with PsA at Week 52, 55.0% at Week 104, and 53.2% at Week 160 (mNRI analysis; N=712).2 Some n values are unavailable due to the imputation method used. **Of patients who entered the OLE at Week 16, 76.7% (546/712) remained on treatment at Week 160.2 †Includes patients originally randomised to placebo.2
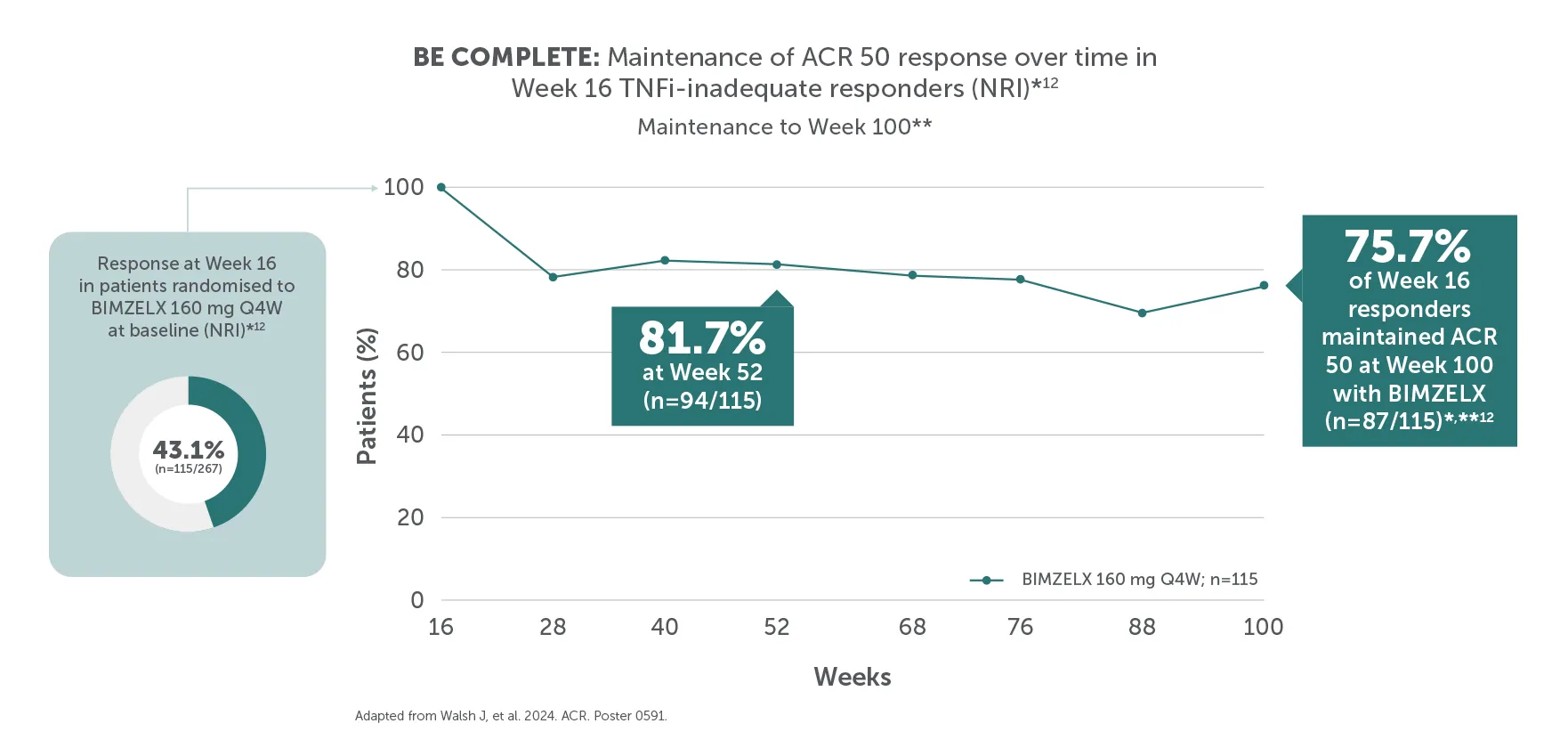
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Data shown here are for patients who completed the phase 3 trial (at Week 16 for BE COMPLETE and Week 52 for BE OPTIMAL) and then entered the BE VITAL open-label extension study.
*In BE COMPLETE, ACR 50 was achieved by 43.1% (n=115/267) at Week 16 and maintained by 75.7% (n=87/115) at Week 100 of TNFI-IR patients (NRI analysis).12 In BE OPTIMAL, ACR 50 was achieved by 43.9% (n=189/431) at Week 16 and maintained by 79.4% (n=150/189) at Week 104 of biologic-naive patients in the BIMZELX treatment arm (NRI analysis).12**Efficacy data for the BE VITAL OLE are reported up to Week 100 for BE COMPLETE and Week 104 for BE OPTIMAL.
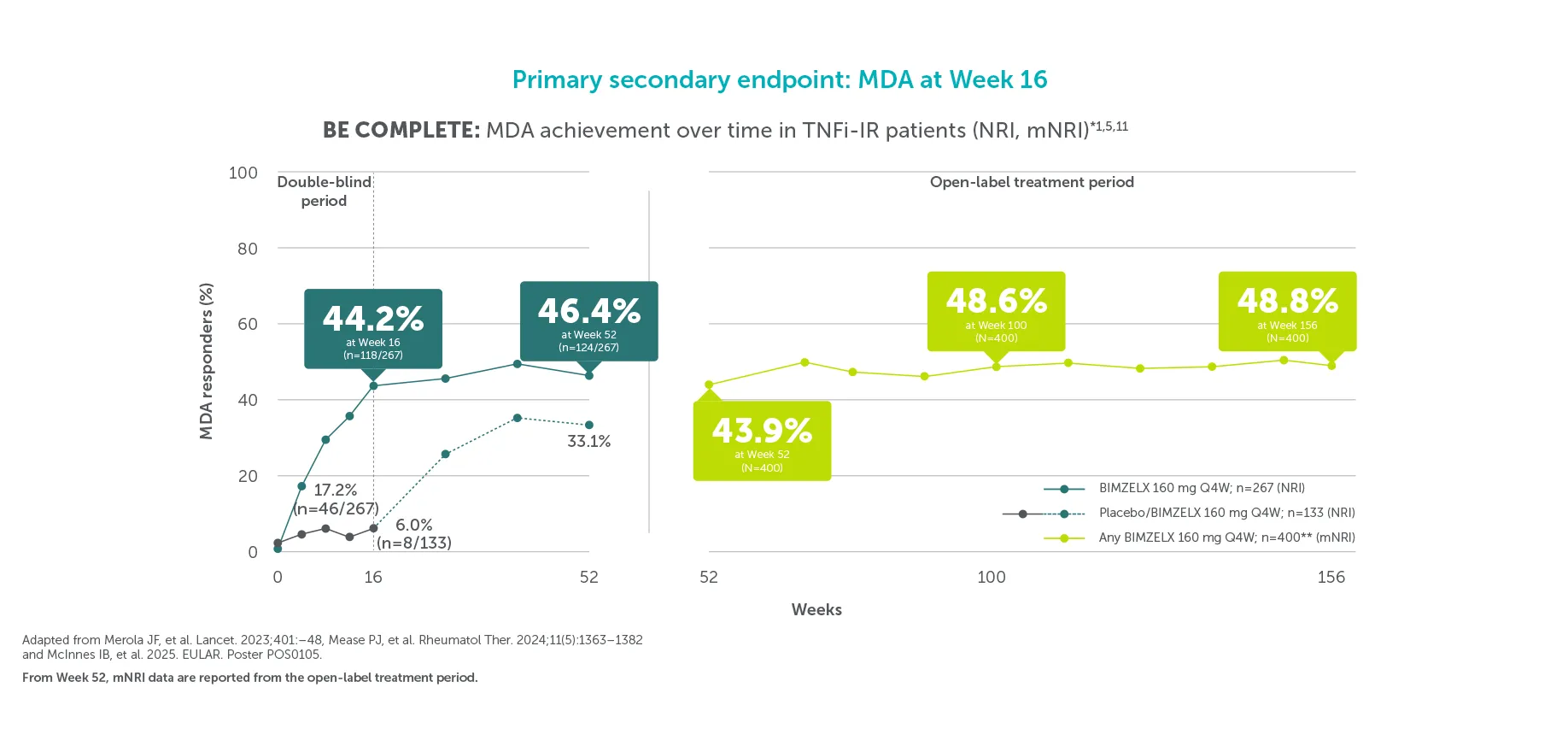
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase 3 trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study. In BE COMPLETE, after Week 16, the investigators and subjects remained blind to the assigned BIMZELX dosing regimen until the final analysis was completed.5
*In BE COMPLETE, MDA was achieved by 17.2% (46/267) of BIMZELX-treated TNFI-IR patients with PsA at Week 4.13 44.2% (118/267) at Week 16,5 and 46.4% (124/267) at Week 52 (NRI analysis).11 In the open-label treatment period, MDA was achieved by 43.9% of BIMZELX-treated TNFI-IR patients with PsA at Week 52. 48.6% at Week 100, and 48.8% at Week 156 (mNRI analysis; N=400).1 Some n values are unavailable due to the imputation method used. **Includes patients originally randomised to placebo.1,5,11
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results.
*In BE OPTIMAL, MDA was achieved by 23.4% (99/431) of BIMZELX-treated biologic- naïve patients with PsA at Week 4.8 45.0% (194/431) at Week 16, and 55.0% (237/431) at Week 52 (NRI analysis).6,8 In the open-label treatment period, MDA was achieved by 56.7% of BIMZELX-treated biologic-naïve patients with PsA at Week 52, 55.0% at Week 104, and 52.9% at Week 160 (mNRI analysis; N=712).2 Some n values are unavailable due to the imputation method used. **BIMZELX is approved for Q4W/Q8W dosing in PsA with coexisting moderate to severe plaque psoriasis.4
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Data shown here are for patients who completed the phase 3 trial (at Week 16 for BE COMPLETE and Week 52 for BE OPTIMAL) and then entered the BE VITAL open-label extension study.
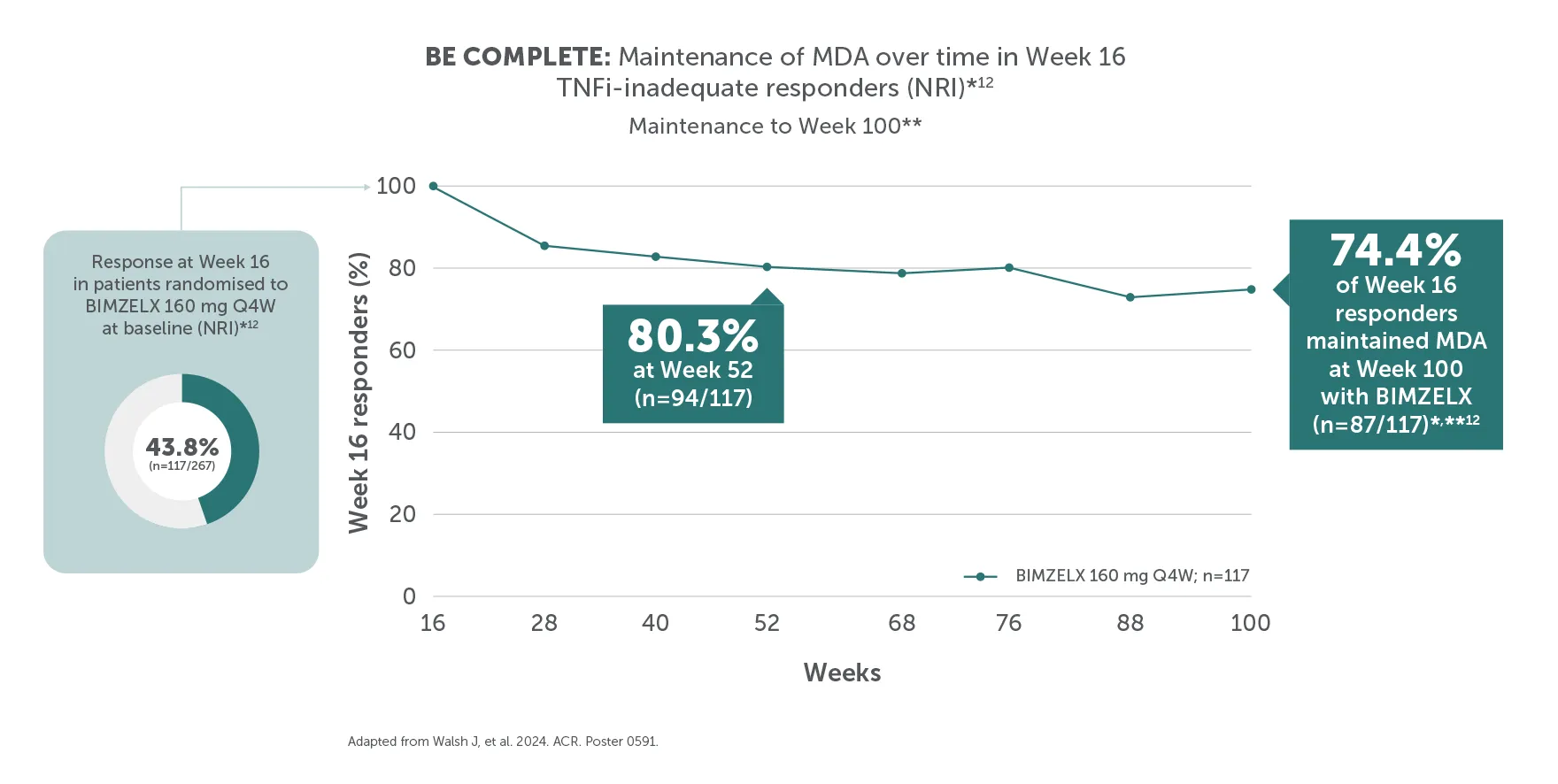
*In BE COMPLETE, MDA was achieved by 43.8% (n=117/267) at Week 16 and maintained by 74.4% (n=87/117) of TNFI-IR patients at Week 100.12 In BE OPTIMAL, MDA was achieved by 45.0% (n=194/431) at Week 16 and maintained by 75.8% (n=147/194) of biologic-naïve patients at Week 104.5,11 **Efficacy data for the BE VITAL OLE are reported up to Week 100 for BE COMPLETE and Week 104 for BE OPTIMAL.
After Week 16, all patients were aware that they were receiving active treatment, which may have affected the results.
*At Week 16, 91.3% (356/390) of biologic-naïve patients in BE OPTIMAL showed no radiographic progression with BIMZELX, vs 88.8% (222/250) with placebo (OC analysis).3,8 At Week 104, 84.2% (282/335) of biologic-naïve patients in BE OPTIMAL showed no radiographic progression with BIMZELX, vs 79.4% (173/218) of biologic-naive patients in the group that switched from placebo to BIMZELX at Week 16 (OC analysis).3
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase 3 trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study. In BE COMPLETE, after Week 16, the investigators and subjects remained blind to the assigned BIMZELX dosing regimen until the final analysis was completed.4
* In BE COMPLETE, PASI 100 was achieved by 58.5% (103/176) at Week 16 (vs 4.5% [4/88] with placebo) of TNF-IR patients in the BIMZELX treatment arm, and 65.9% (116/176) at Week 52 (NRI analysis).5,11 In the open-label treatment period, PASI 100 was achieved by 66.2% at Week 52, 67.5% at Week 100, and 67.5% at Week 156 of TNFI-IR patients in the BIMZELX treatment arm (mNRI analysis; N=264).1 Some n values are unavailable due to the imputation method used. **PASI response in patients with psoriasis involving ≥3% BSA at baseline.1,5,11 †Includes patients originally randomised to placebo.1 BIMZELX is approved for Q4W/Q8W dosing in PsA with coexisting moderate to severe plaque psoriasis.4
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results. Some n values are not available due to imputation method used. *Data pooled from BE COMPLETE and BE OPTIMAL6 **Week 156 data from patients who completed the BE COMPLETE phase 3 trial and then entered the BE VITAL open-label extension study.1 †Week 160 data from patients who completed the BE OPTIMAL phase 3 trial and then entered the BE VITAL open-label extension.2
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results. *Data pooled from BE COMPLETE and BE OPTIMAL6 **Week 156 data from patients who completed the BE COMPLETE phase 3 trial and then entered the BE VITAL open-label extension study.1 †Week 160 data from patients who completed the BE OPTIMAL phase 3 trial and then entered the BE VITAL open-label extension.2
After Week 16, patients in BE COMPLETE and BE OPTIMAL were aware that they were receiving active treatment, which may have affected the results. Some n values are not available due to imputation method used. *Week 156 data from patients who completed the BE COMPLETE phase 3 trial and then entered the BE VITAL open-label extension study.6 **Week 160 data from patients who completed the BE OPTIMAL phase 3 trial and then entered the BE VITAL open-label extension.2
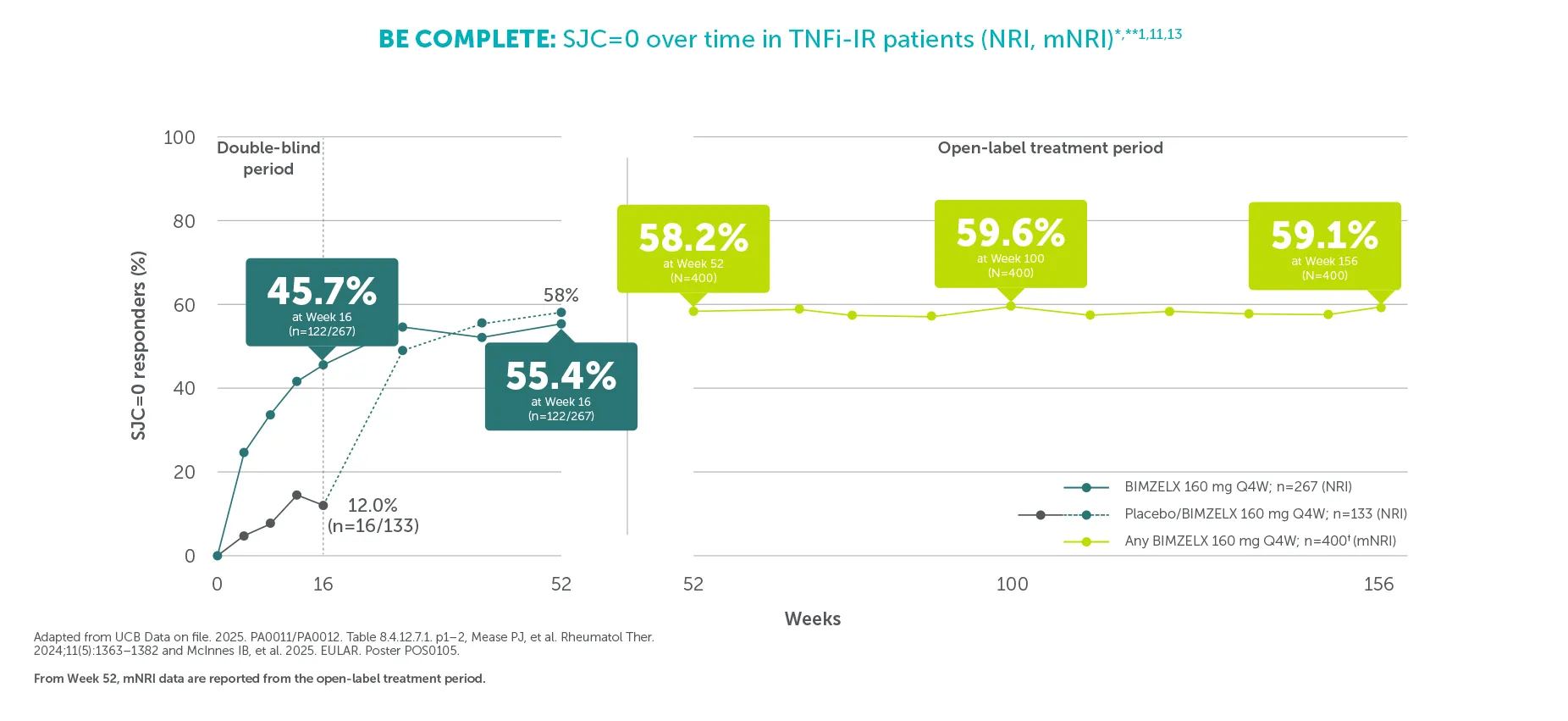
Efficacy outcomes are reported from the BE OPTIMAL and BE COMPLETE trials and combined open-label treatment period following Week 52 of BE OPTIMAL and Week 16 of BE COMPLETE. After Week 16, all patients were aware that they were receiving active treatment, which may have affected the results. *In BE COMPLETE, SJC=0 was achieved by 45.7% (122/267) at Week 16 (vs 12% [16/133] with placebo) (NRI analysis).13 In the open-label treatment period, SJC=0 was achieved by 58.2% at Week 52, 59.6% at Week 100, and 59.1% at Week 156 of TNF-IR patients in the BIMZELX treatment arm (mNRI analysis; N=400).1 Some n values are unavailable due to the imputation method used. **SJC ranges from 0-66. †Includes patients originally randomised to placebo.1,13
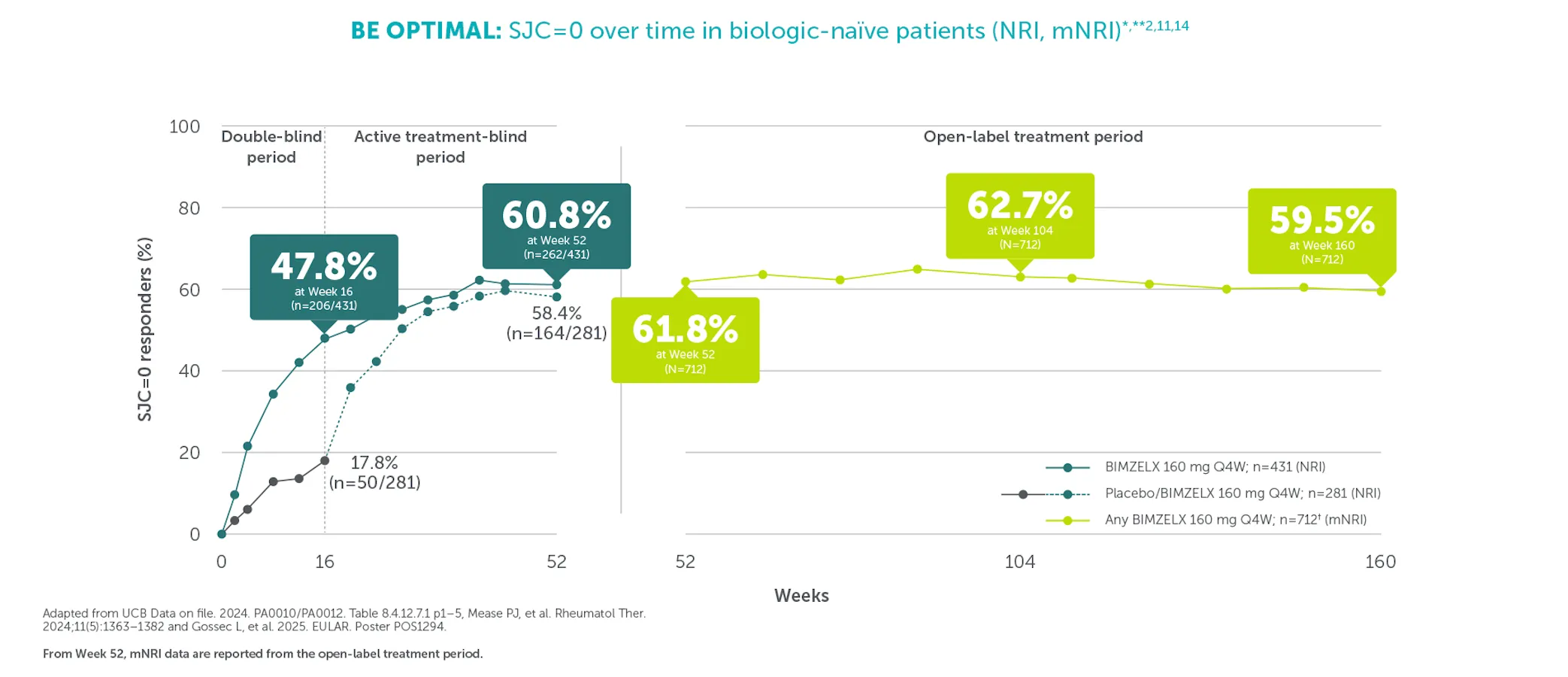
Efficacy outcomes are reported from the BE OPTIMAL and BE COMPLETE trials and combined open-label treatment period following Week 52 of BE OPTIMAL and Week 16 of BE COMPLETE. After Week 16, all patients were aware that they were receiving active treatment, which may have affected the results. *In BE OPTIMAL, SJC=0 was achieved by 47.8% (206/431) at Week 16 (vs 17.8% [50/281] with placebo), and 60.8% (262/431) at Week 52 (vs 58.4% [164/281] with placebo) of biologic-naïve patients in the BIMZELX treatment arm (NRI analysis).11,14 In the open-label treatment period, SJC=0 was achieved by 61.8% at Week 52, 62.7% at Week 104, and 59.5% at Week 160 of biologic-naïve patients in the BIMZELX treatment arm (mNRI analysis; N=712).2 Some n values are unavailable due to the imputation method used. **SJC ranges from 0-66.2 †Includes patients originally randomised to placebo.2,12
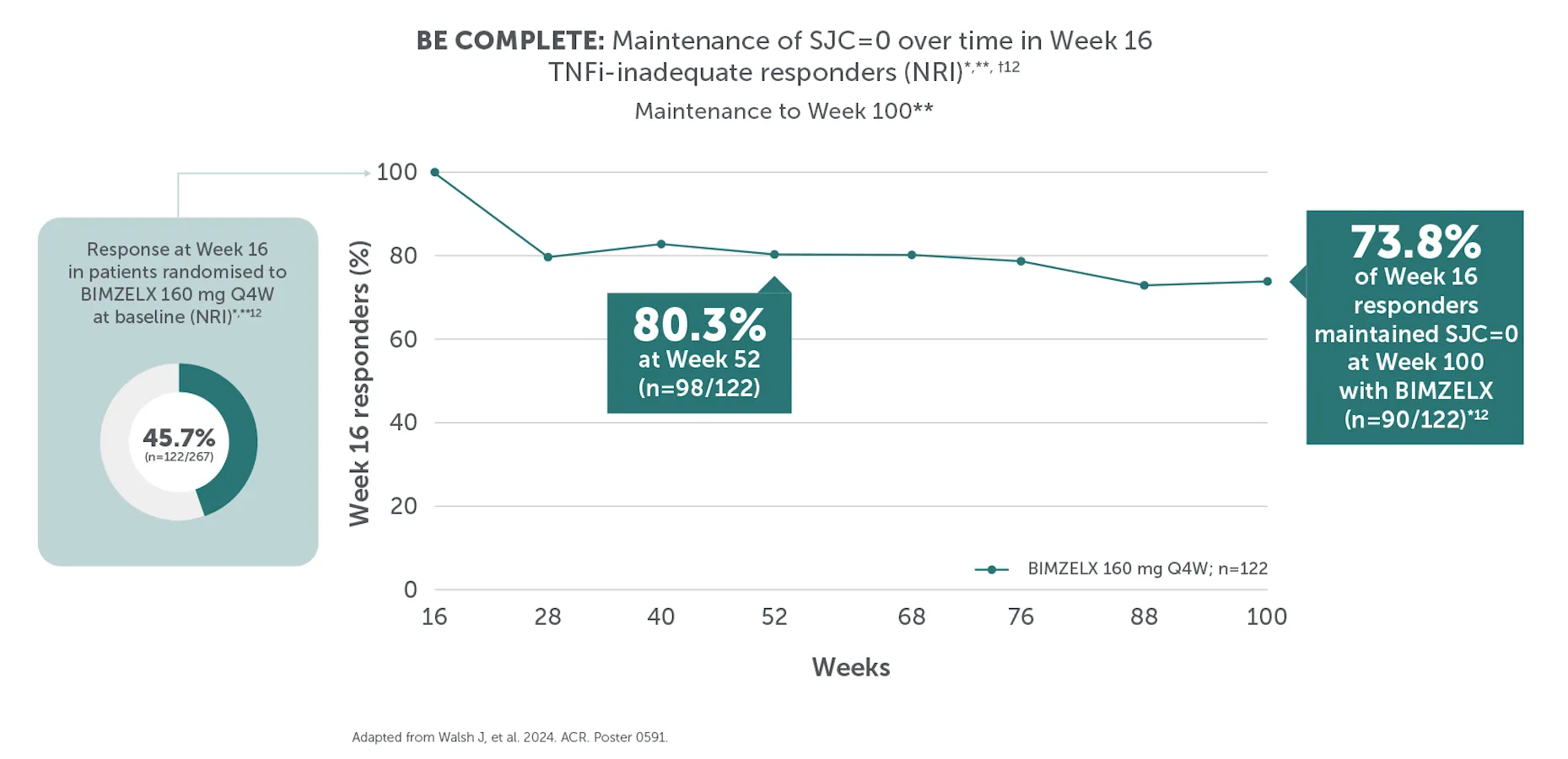
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Data shown here are for patients who completed the phase 3 trial (at Week 16 for BE COMPLETE and Week 52 for BE OPTIMAL) and then entered the BE VITAL open-label extension study. *In BE COMPLETE, SJC=0 was achieved by 45.7% (n=122/267) at Week 16 and maintained by 73.8% (n=90/122) of TNFI-IR patients at Week 100.12 In BE OPTIMAL, SJC=0 was achieved by 47.8% (n=206/431) at Week 16 and maintained by 75.2% (n=155/206) of biologic-naïve patients at Week 104.12 **SJC ranges from 0-66.12 †Efficacy data for the BE VITAL OLE are reported up to Week 100 for BE COMPLETE and Week 104 for BE OPTIMAL.
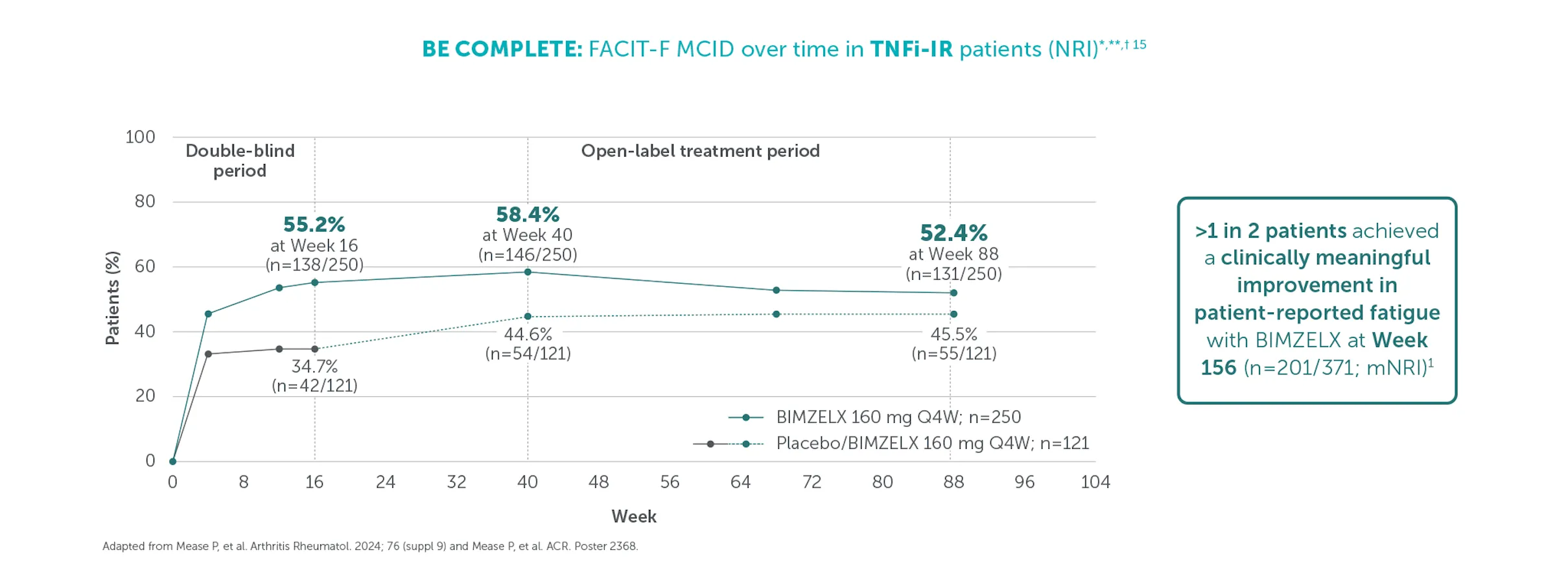
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Data shown here are for patients who completed the phase 3 trial at Week 16 for BE COMPLETE and then entered the BE VITAL open-label extension study. *FACIT-F scores range from 0-52, with lower scores indicating worse fatigue.15FACIT-F MCID, representing minimal clinically meaningful improvement, is defined by a >4-point score improvement from baseline in patients with FACIT-F ≤48 at baseline.15 Change from baseline in FACIT-F was an additional efficacy outcome in BE COMPLETE at Week 16.16**In BE COMPLETE, FACIT-F MCID was achieved by 58.4% (146/250) at Week 40, 52.4% (131/250) at Week 88 of TNFI-IR patients in the BIMZELX treatment arm (NRI analysis),17 and 54.2% (201/371) in the any BIMZELX group at Week 156 (mNRI analysis).1 †FACIT-F data were collected at Week 40 and Week 88 in BE COMPLETE.17
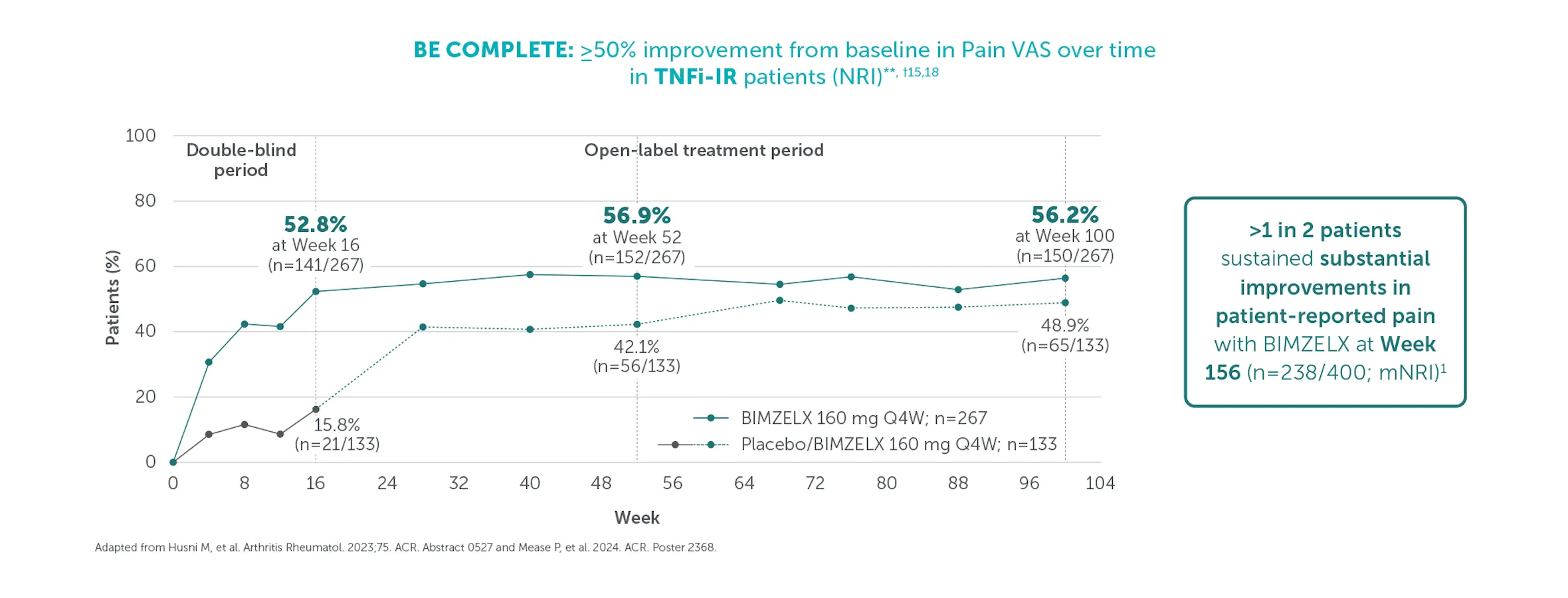
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Data shown here are for patients who completed the phase 3 trial at Week 16 for BE COMPLETE and then entered the BE VITAL open-label extension study. *Arthritis pain was assessed using a 100-point scale where higher patient-reported scores indicate worse status. A clinically meaningful improvement in Pain VAS score was defined as a ≥30% improvement from baseline. A substantial improvement in Pain VAS score was defined as a ≥50% improvement from baseline.15 Change from baseline in Patient's Assessment of Arthritis Pain was an additional efficacy outcome in BE COMPLETE at Week 16.5**In BE COMPLETE, ≥50% improvement in Pain VAS was achieved by 52.8% (141/267) at Week 16 (vs 15.8% [21/133] with placebo), 56.9% (152/267) at Week 52, 56.2% (150/267) at Week 100 (NRI analysis),15,18 and 59.4% of patients in the any BIMZELX group at Week 156 (mNRI analysis).1 †In BE COMPLETE, data are reported to Week 100 as some patients had not completed Week 104 at time of reporting.
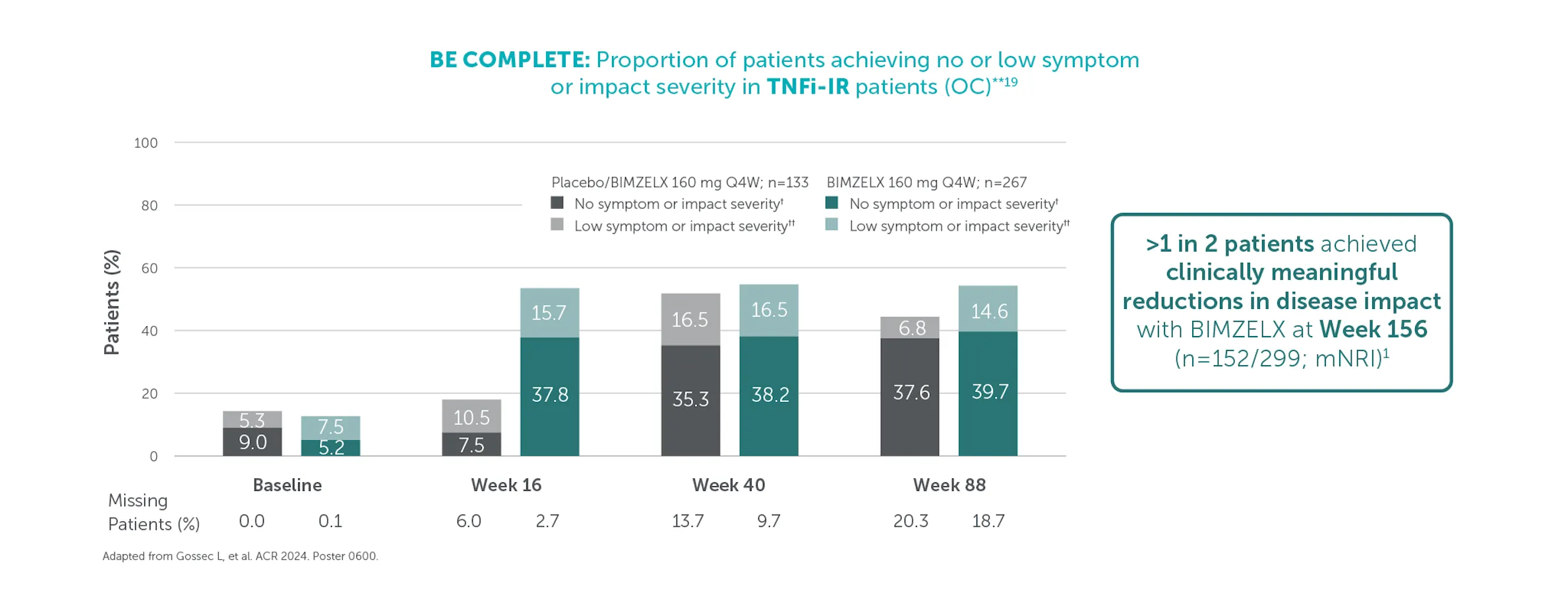
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Data shown here are for patients who completed the phase 3 trial at Week 16 for BE COMPLETE and then entered the BE VITAL open-label extension study. *Randomised set. PsAID-12 scores range from 0-10; higher scores indicate worse status.19 Change from baseline in PsAID-12 was an additional efficacy outcome in BE COMPLETE at Week 16.5 **In BE COMPLETE, PsAID-12 was reported at Baseline, Week 16 Week 40 and Week 88.19 †No symptom or impact severity defined as PsAID-12 total score ≤1.15 ††Low symptom or impact severity defined as PsAID-12 total score >1.15 to ≤1.95.19 Clinically meaningful improvement response: ≥3-point decrease from baseline when respective PsAID-12 score was ≥3 at baseline.19
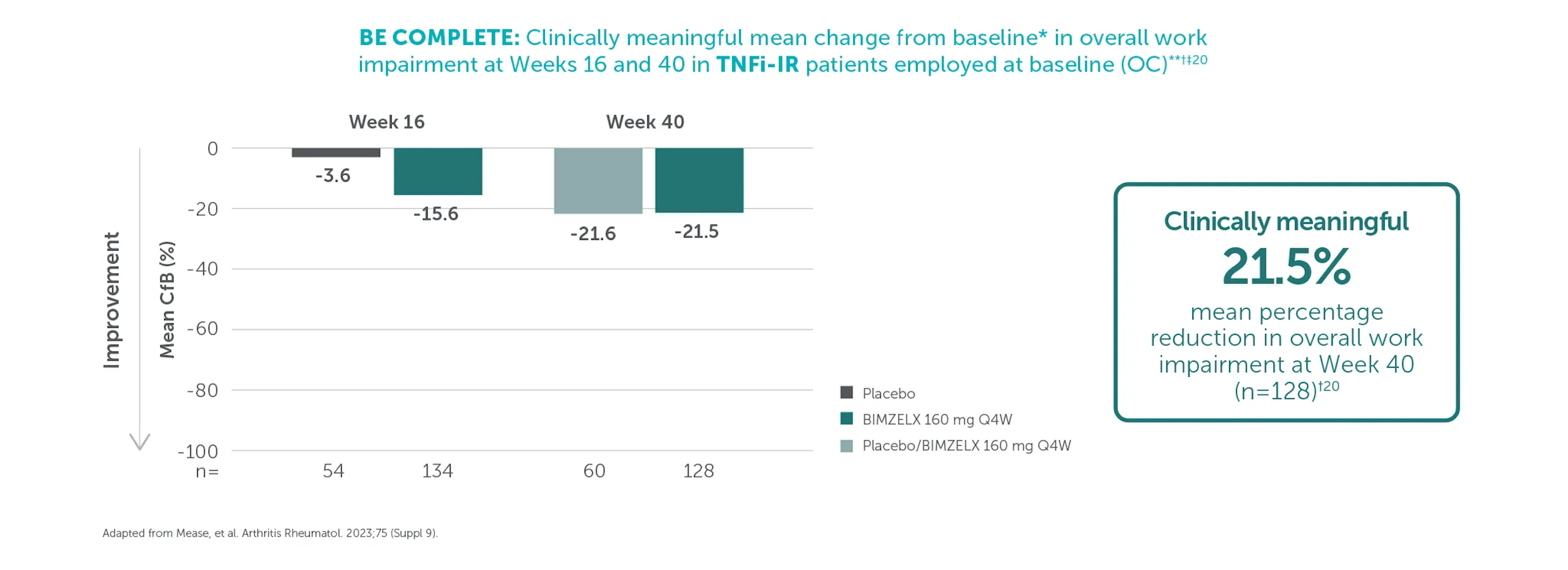
Week 52 data shown here are for patients who completed the BE COMPLETE phase 3 trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study. After Week 16, all patients were aware that they were receiving active treatment, which may have affected the results. *At baseline, 40.7% (n=158) of patients in the BIMZELX treatment arm experienced overall work impairment, vs 40.3% (n=73) in the placebo arm. **Mean percentage reduction from baseline in overall work impairment was 15.6% (n=134) at Week 16 (vs 3.6% [n=54] with placebo), and 21.5% (n=128) at Week 40 of TNFI-IR patients in the BIMZELX treatment arm (vs 21.6% [n=60] in the group that switched from placebo to BIMZELX 160 mg Q4W at Week 40; OC analyses).20 †Clinically meaningful improvement in overall work impairment was estimated to be 15%.10,20 ‡In BE COMPLETE, percentage employment at baseline was 64.0% (n=171/267) of patients in the BIMZELX treatment arm and 58.6% (n=78/133) in the placebo arm.20
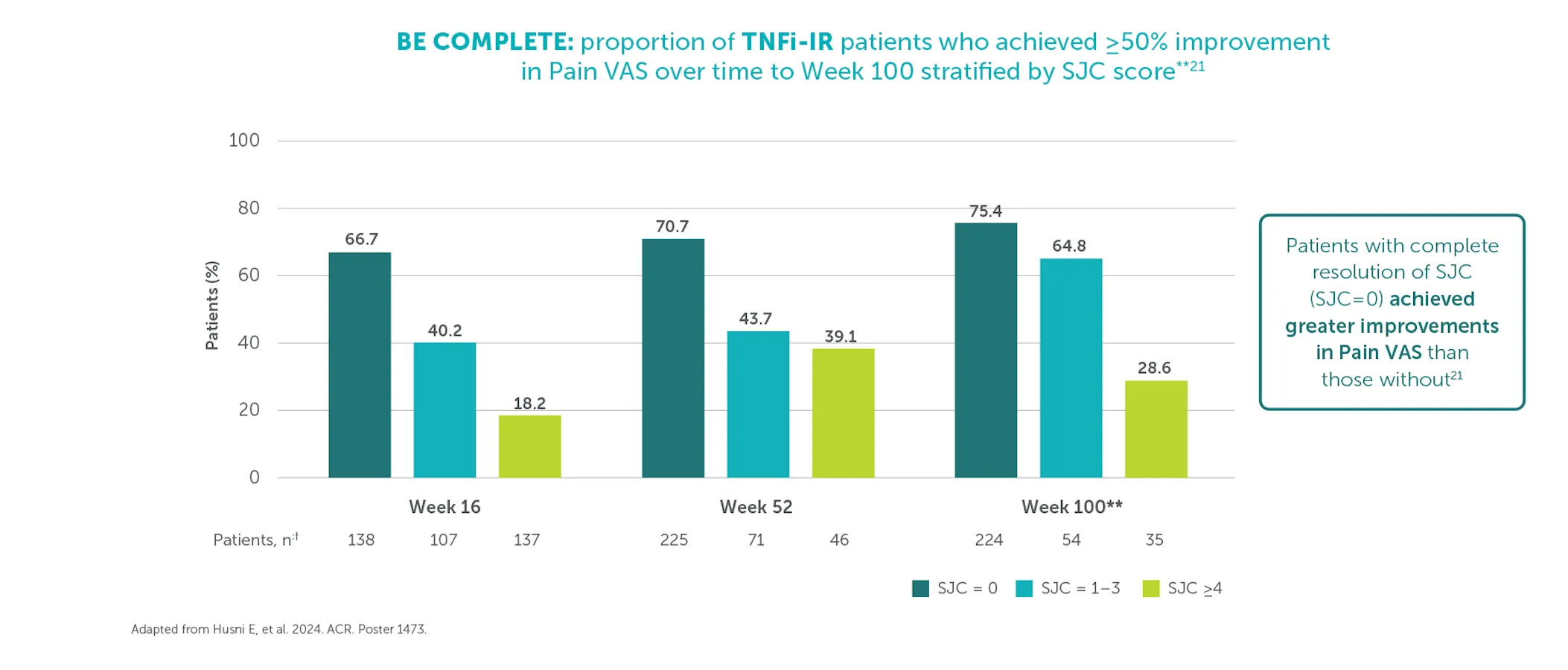
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Data shown here are for patients who completed the phase 3 trial (at Week 16 for BE COMPLETE and Week 52 for BE OPTIMAL) and then entered the BE VITAL open-label extension study. *Arthritis pain was assessed using a 100-point scale where a patient-reported score of 0 indicates no pain and 100 indicates most severe pain.15 A substantial improvement in Pain VAS score was defined as a ≥50% improvement from baseline. Lower SJC scores indicate greater improvements with a score of 0 indicating complete resolution.21 **In BE COMPLETE, data are reported to Week 100 as some patients had not completed Week 104 at time of reporting. †Pooled patient population including patients originally randomised to placebo.
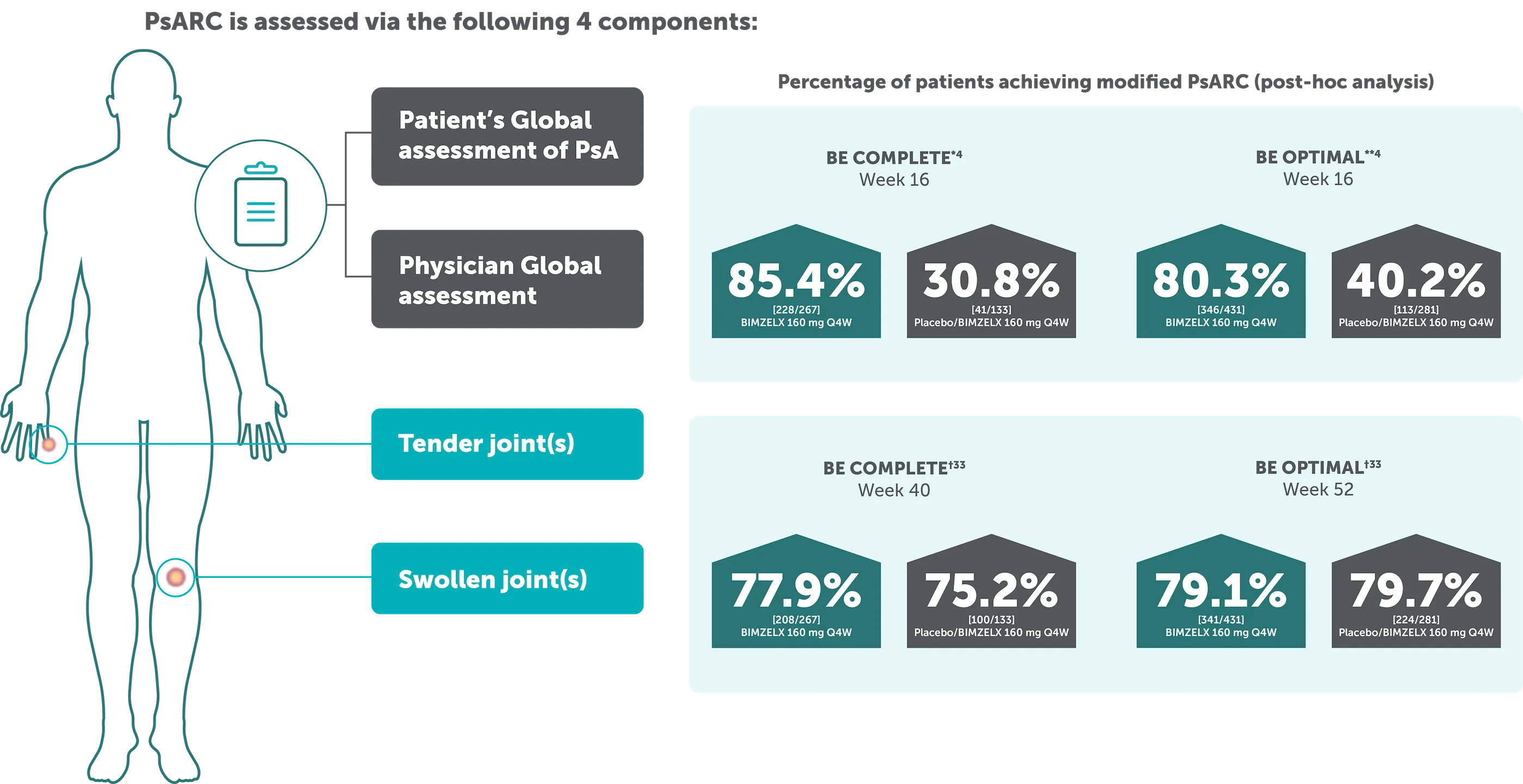
*The proportion of patients achieving modified PsARC at Week 16 was also higher in BE COMPLETE (85.4% vs 30.8% respectively).4 **BE OPTIMAL: The proportion of patients achieving modified PsARC at Week 16 was higher in the bimekizumab-treated patients compared to placebo (80.3% vs 40.2% respectively).4 †79.1% (341/431) of biologic-naïve patients in BE OPTIMAL and 77.9% (208/267) of TNF-IR patients in BE COMPLETE achieved PsARC with BIMZELX at Week 52 and at Week 40, respectively (NRI analysis).33
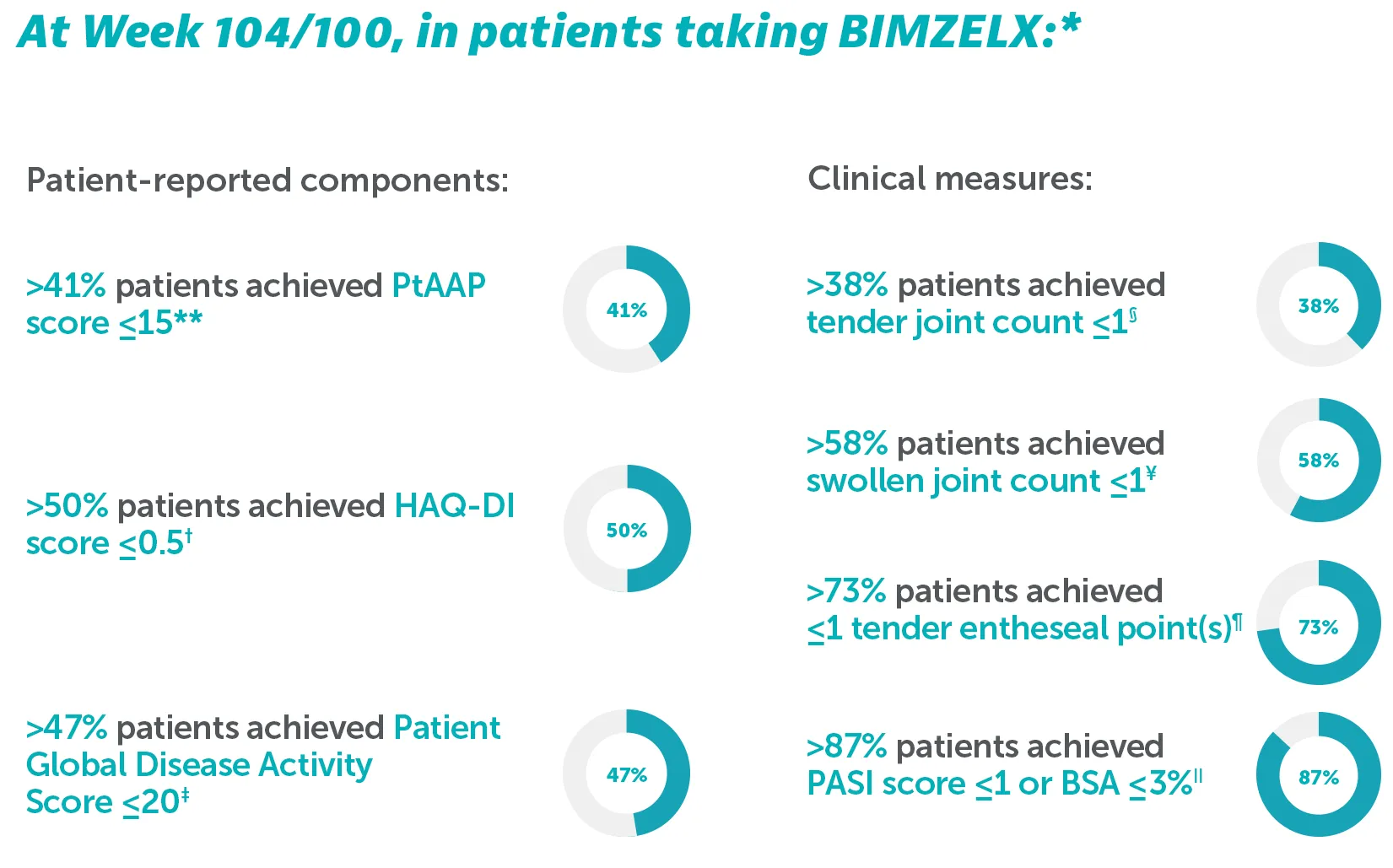
*Outcomes are reported to Week 104 for BE OPTIMAL and Week 100 for BE COMPLETE as some patients had not yet completed their Week 104 visit at time of reporting.34
**In BE OPTIMAL at Week 104, PtAAP ≤15 was achieved by 45.7% (n=197/431) of biologic-naïve patients; In BE COMPLETE at Week 100, PtAAP ≤15 was achieved by 41.9% (n=112/267) of TNF-IR patients.34 †In BE OPTIMAL at Week 104, HAQ-DI ≤0.5 was achieved by 54.1% (n=233/431) of biologic-naïve patients; In BE COMPLETE at Week 100, HAQ-DI ≤0.5 was achieved by 50.6% (n=136/267) of TNFI-IR patients.34 ‡In BE OPTIMAL at Week 104, Patient Global Disease Activity Score ≤20 was achieved by 51.0% (n=220/431) of biologic-naïve patients; In BE COMPLETE at Week 100, Patient Global Disease Activity Score ≤20 was achieved by 47.6% (n=127/267) of TNFI-IR patients.34 §In BE OPTIMAL at Week 104, TJC ≤1 was achieved by 46.4% (n=200/431) of biologic-naïve patients; In BE COMPLETE at Week 100, TJC ≤1 was achieved by 38.2% (n=102/267) of TNF-IR patients.34 ɎIn BE OPTIMÁL at Week 104, SJC ≤1 was achieved by 67.7% (n=292/431) of biologic-naïve patients; In BE COMPLETE at Week 100, SJC ≤1 was achieved by 58.8% (n=157/267) of TNF-IR patients.34 ¶In BE OPTIMAL at Week 104, LEI ≤1 achieved by 74.7% (n=318/431) of biologic-naïve patients; In BE COMPLETE at Week 100, LEI ≤1 was achieved by 73.0% (n=195/267) of TNFI-IR patients.34 IIIn BE OPTIMAL at Week 104, PASI ≤1/BSA ≤3% was achieved by 89.3% (n=385/431) of biologic-naïve patients, In BE COMPLETE at Week 100, PASI ≤1/BSA ≤3% was achieved by 87.6% (n=234/267) of TNFI-IR patients.34
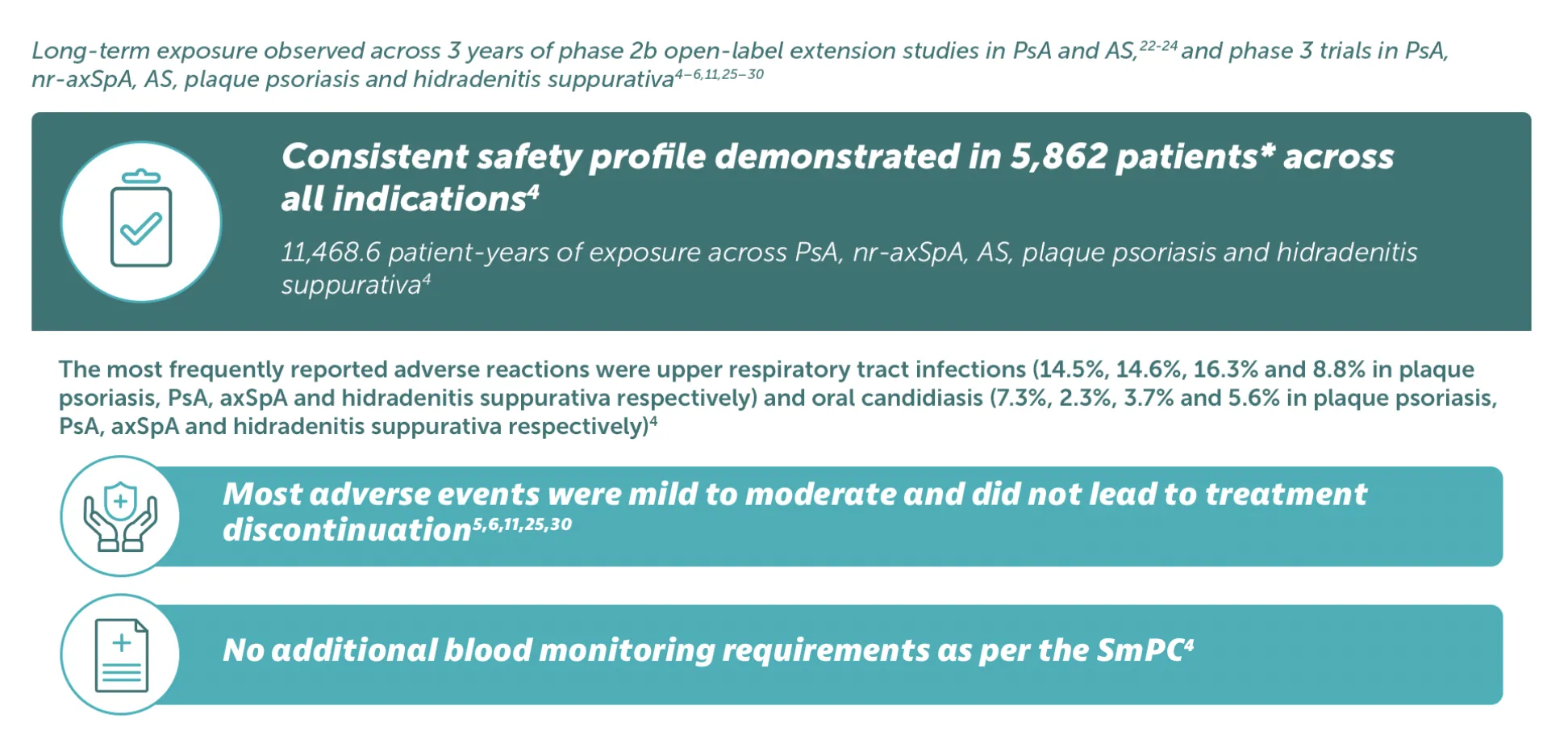
Adverse events: Refer to SmPC for full information. Very common (≥1/10): Upper respiratory tract infection; Common (≥1/100 to< 1/10): Oral candidiasis, tinea infections, ear infections, herpes simplex infections, oropharyngeal candidiasis, gastroenteritis, folliculitis, headache, dermatitis and eczema, acne, injection site reactions, fatigue; Uncommon (≥1/1,000 to<1/100): Mucosal and cutaneous candidiasis (including oesophageal candidiasis), conjunctivitis, neutropenia, inflammatory bowel disease. *5,862 patients treated in blinded and open-label clinical studies in PsA, nr-axSpA, AS, moderate to severe plaque psoriasis, and moderate to severe HS. Of these, over 4,660 patients were exposed to BIMZELX for at least one year.4
BIMZELX is generally well tolerated in patients with axSpA and PsA as seen by long-term exposure analyses from phase 2b/3 trials in patients with at least 104 weeks of total study participation31
Pooled analysis of patients with PsA:
Overview of TEAEs up to data-cut
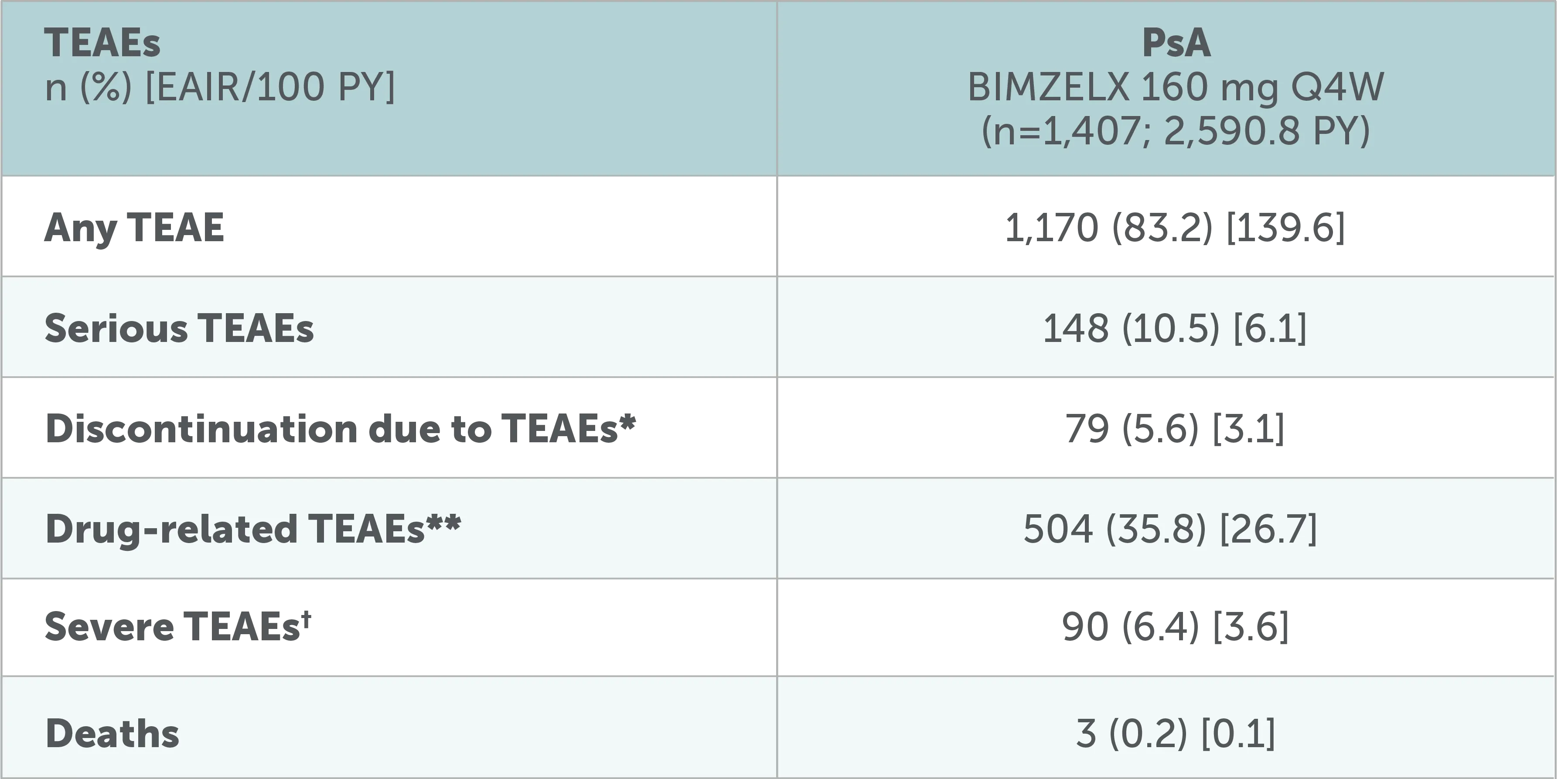
Adapted from Mease P, et al. RMD Open. 2025;11(2):e005026
Data to the July 2022 data-cut shown, including all patients who received ≥1 dose of BIMZELX 160 mg Q4W in the phase 2b/3 studies. After Week 16, all patients were aware that they were receiving active treatment, which may have affected the results. *Including TEAEs leading to death.31 **Per investigator assessment. 31†The intensity of TEAEs was assessed by the investigators as 'mild', 'moderate' or 'severe, independently from seriousness.
Pooled analysis of patients with PsA:
Overview of AEs of special monitoring up to data-cut
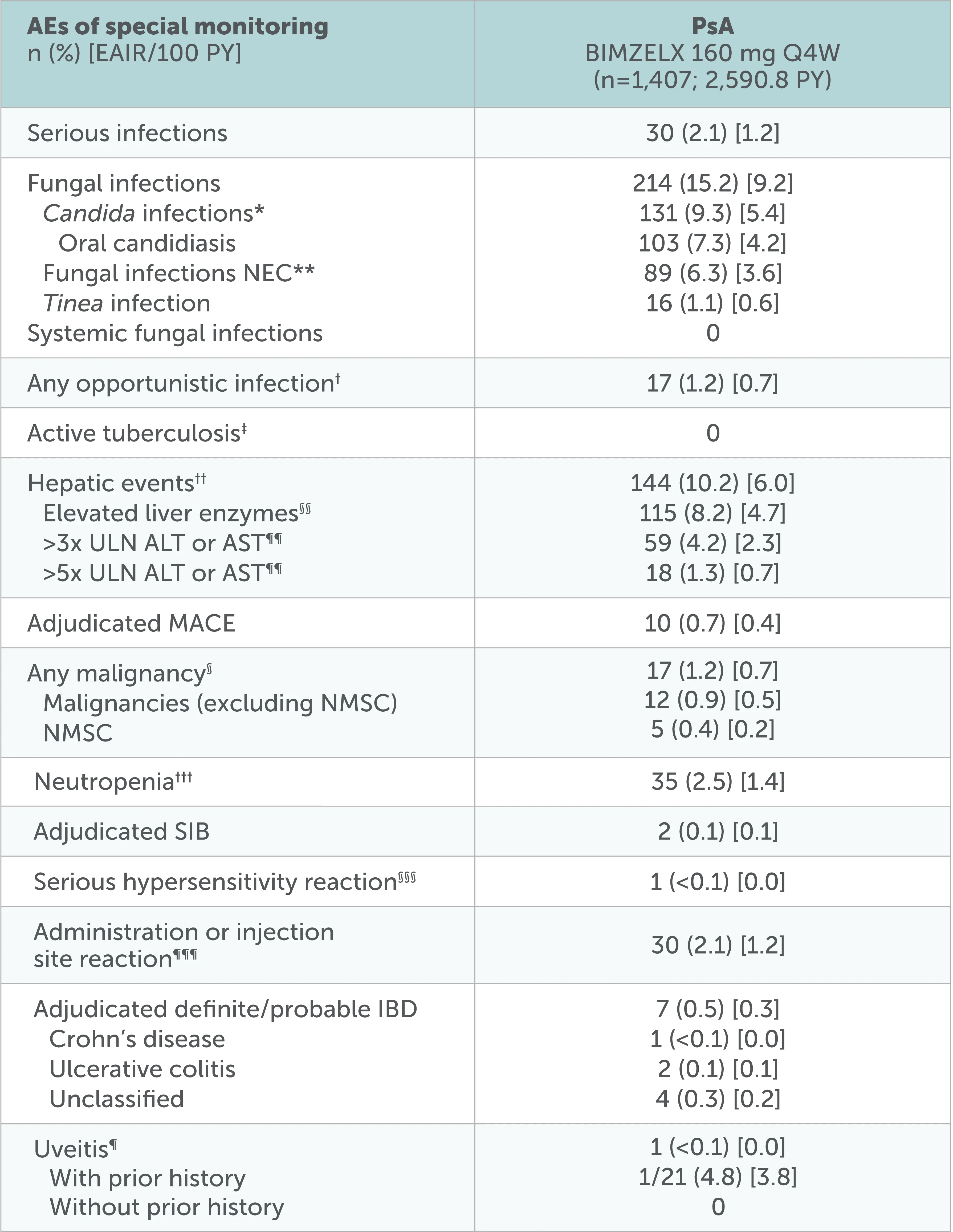
Adapted from Mease P, et al. RMD Open. 2025;11(2):e005026
Data to the July 2022 data-cut shown, including all patients who received ≥1 dose of BIMZELX 160 mg Q4W in the phase 2b/3 studies. After Week 16, all patients were aware that they were receiving active treatment, which may have affected the results. *Shown by MedDRA preferred term in online supplemental table 2.31 **NEC denotes groupings of miscellaneous terms that do not readily fit into other hierarchical classifications within a specific SOC in the MedDRA.31 †Not including one serious case of oropharyngeal candidiasis in a patient with PSA, which was identified as an opportunistic infection after the July 2022 data-cut.31 ‡At baseline, 46 (5.4%) patients with axSpA and 34 (2.4%) patients with PsA had a history of ongoing/latent tuberculosis (phase 2b/3 pool).31 §Identified using the SMQ ‘Malignant tumours’.31 ¶Includes the preferred terms ‘Autoimmune uveitis’, ‘Iridocyclitis', 'Iritis' and 'Uveitis’.31 ††Includes events in the SMQ 'Drug-related hepatic disorders-comprehensive search’ excluding the sub-SMQS 'Liver neoplasms, benign (including cysts and polyps)' and 'Liver neoplasms, malignant and unspecified’.31 §§Elevated liver enzymes include the following preferred terms reported as adverse events: Increased/abnormal levels of ALT, AST, Blood bilirubin, Gamma-glutamyltransferase, Hepatic enzyme, Liver Function test or Transaminases.31 ¶¶n=411 for axSpA; n=1405 for PsA. †††Includes preferred terms identified based on UCB-defined search criteria.31 §§§Hypersensitivity reactions identified via the SMQ ‘Hypersensitivity’.31 ¶¶¶Identified using the HLTS 'Administration site reactions NEC' and 'Injection site reactions'.31
No new safety signals were reported31
The three most common TEAEs were SARS-COV-2 (COVID-19) infection, nasopharyngitis, and upper respiratory tract infection
Incidence rate of oral candidiasis decreased over time and infrequently led to discontinuation
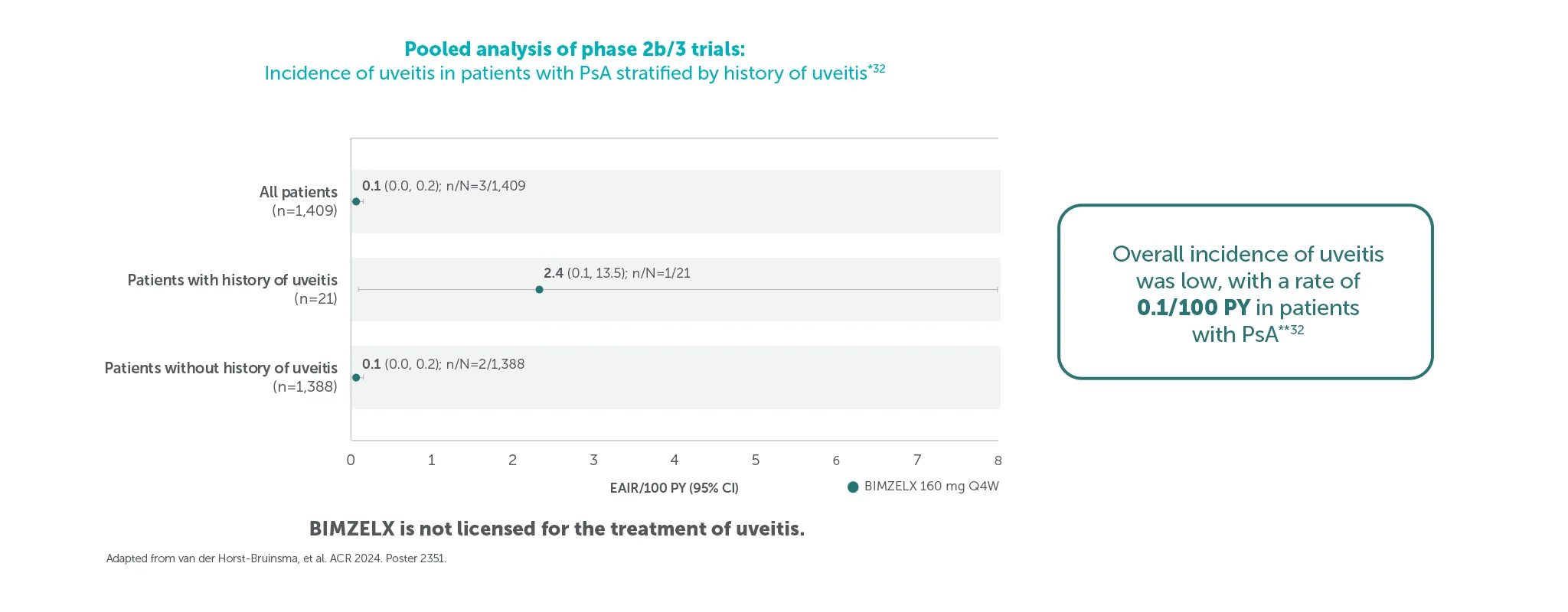
Pooled safety set including all patients who received ≥1 dose of BIMZELX 160 mg Q4W in the phase 2b/3 studies. Uveitis rates and EAIRs/100 PY were reported over median durations of approximately 2.8 years (axSpA) and 2.7 years (PsA); the data cut-off for both patient populations was set at July 2023.32 *Data shown are from the July 2023 data cut.32 Duration by data-cut is varied between patients, depending on feeder study duration and initial randomisation.32 Overall exposure across the pooled phase 2b/3 trials was 3,656 PY.32**All uveitis events were mild or moderate and no events led to treatment discontinuation.32
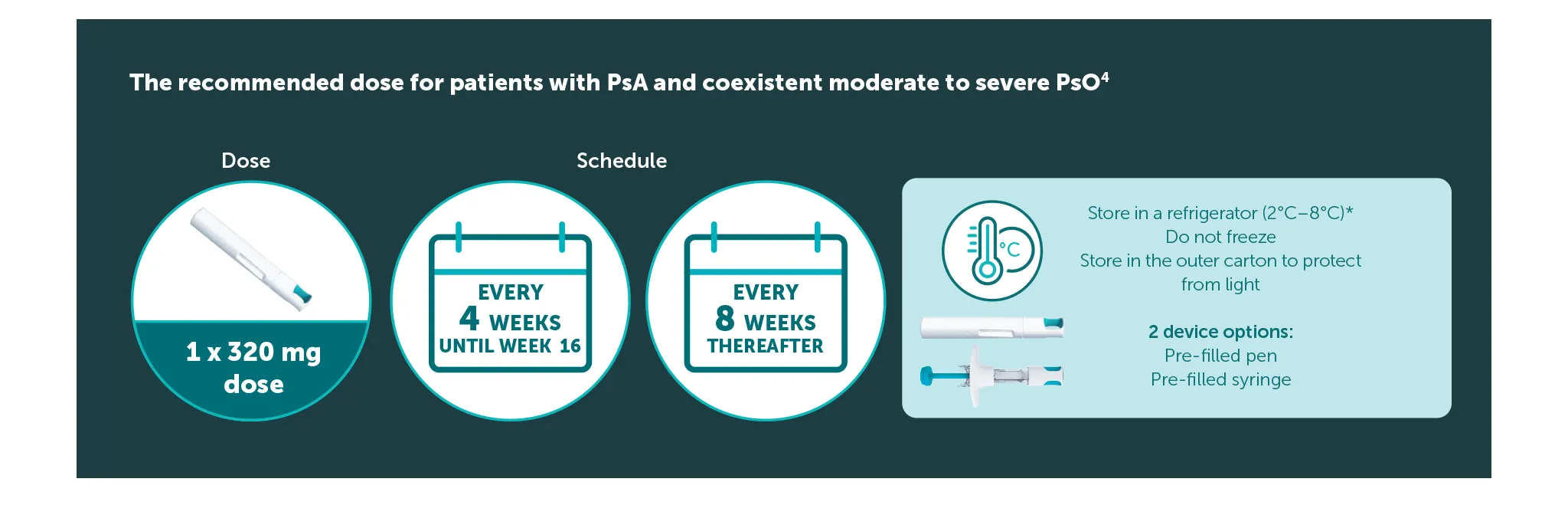
The recommended dose for adult patients with PsA and coexistent moderate to severe PsO is 320 mg (given as two subcutaneous injections of 160 mg or one subcutaneous injection of 320 mg) at Weeks 0, 4, 8, 12, 16, and every 8 weeks thereafter.4 After 16 weeks, regular assessment of efficacy is recommended and if sufficient clinical response in joints cannot be maintained, a switch to 160 mg every 4 weeks can be considered. 4 Consideration should be given to discontinuing treatment in patients who have shown no improvement by 16 weeks of treatment. 4 For patients with a body weight ≥120 kg who do not achieved complete skin clearance at Week 16, 320 mg every 4 weeks after Week 16 may further improve treatment response.4
*The pre-filled syringe or pen may be stored at room temperature (up to 25 °C) for up to 25 days. Once removed from the refrigerator and stored under these conditions, discard after 25 days or by the expiry date printed on the container, whichever occurs first. A field for the date is provided on the carton to record the date removed from the refrigerator.4
Clinical study designs
Ranked secondary endpoints at Week 16 were: Change from baseline in Health Assessment Questionnaire-Disability Index total score; 90.0% or greater improvement in PASI scores in patients with baseline psoriasis affecting 3.0% or more BSA; change from baseline in SF-36 Physical Component Summary norm-based score: proportion of patients achieving MDA response; change from baseline in van der Heijde-modified Total Sharp Score in patients with one resolution of dactylitis; resolution of enthesitis assessed using the LEI, Dactylitis Index; change from baseline in van der Heijde-modified Total Sharp Score in the overall radiographic set.6
Ranked secondary endpoints were: Change from baseline in Health Assessment Questionnaire-Disability Index total score; the proportion of patients achieving 90.0% or greater improvement in PASI scores in patients with baseline psoriasis affecting 3.0% or more BSA; change from baseline in SF-36 Physical Component Summary norm-based score; proportion of patients achieving MDA response.5
IE-BK-2400114
Date of creation: October 2025