Image

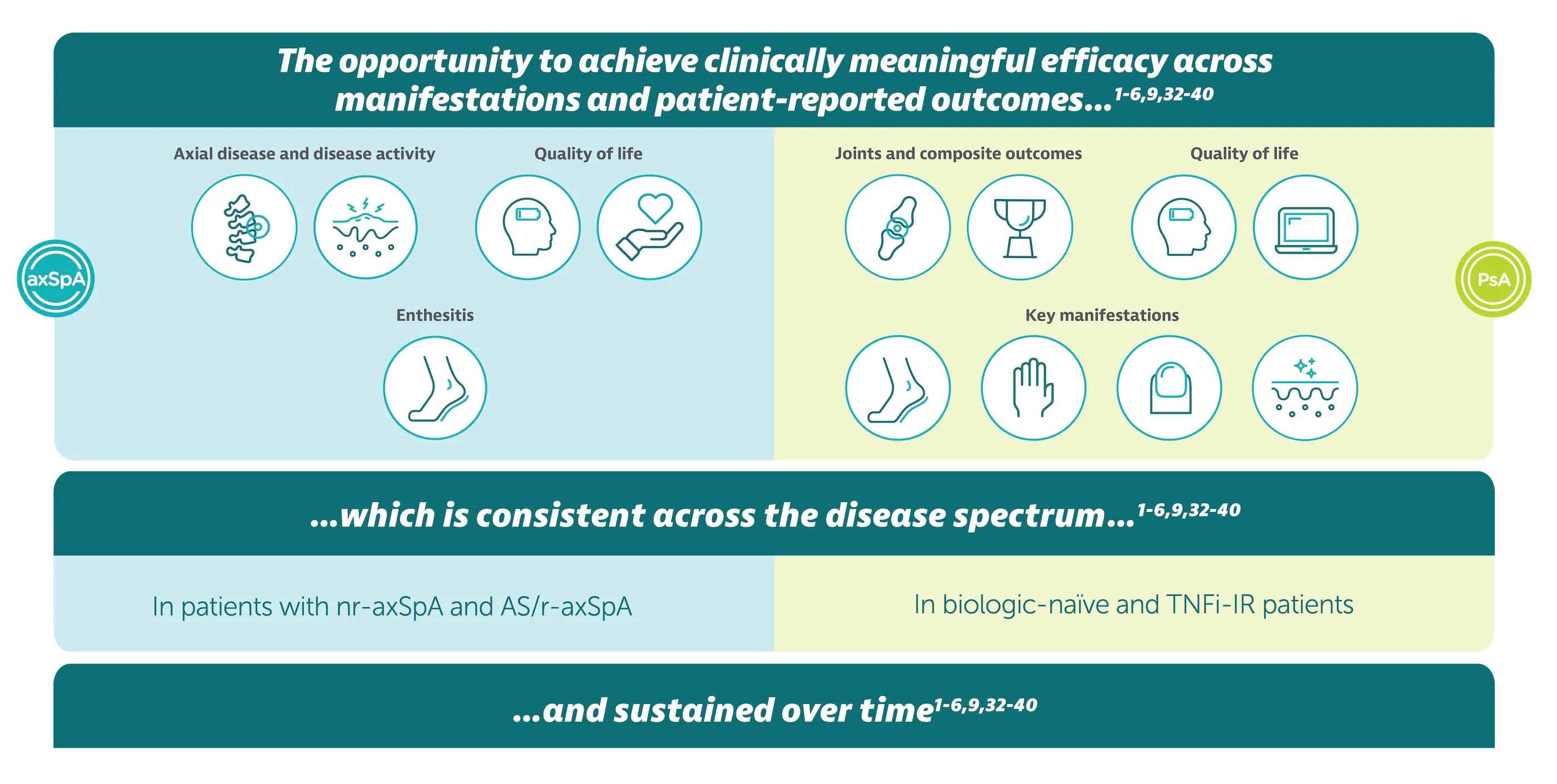
*Efficacy across manifestations means ACR 50 and PASI 90 for PsA, ASAS 40 and ASDAS <2.1 for axSpA. ACR 50 achieved by 43.9% (189/431) biologic-naïve and 43.4% (116/267) TNFi-IR patients with PsA at Week 16 (primary endpoint in BE OPTIMAL and BE COMPLETE; vs 10.0% (28/281) and 6.8% (9/133) with placebo, respectively; p<0.001),1–3 54.5% (235/431) and 51.7% (138/267) at Week 52, respectively (NRI analysis).4,5 ASAS 40 achieved by 47.7% (61/128) nr-axSpA patients and 44.8% (99/221) AS patients at Week 16, (primary endpoint in BE MOBILE 1/2; vs 21.4% (27/126) and 22.5% (25/111) with placebo, respectively; p<0.001);6 60.9% (78/128) and 58.4% (129/221) at Week 52, respectively (NRI analysis).3 Rapid onset demonstrated by numerically higher responder rates (ACR 50) observed vs placebo at Week 4 in BE OPTIMAL, 17.6% (76/431) vs 3.2% (9/281); and in BE COMPLETE, 16.1% (43/267) vs 1.5% (2/133), respectively (both nominal p<0.001).1–3 At Week 4, PASI 90 responses were numerically greater in BIMZELX-treated patients vs placebo in BE OPTIMAL, 19.8% (43/217) vs 4.3% (6/140), and in BE COMPLETE, 26.7% (47/176) vs 0% (0/88), respectively.1,2 At Week 52, PASI 90 achieved by 71.4% (155/217) and 74.4% (131/176) of BIMZELX-treated patients in BE OPTIMAL and BE COMPLETE, respectively (ranked secondary endpoint, NRI analysis; PASI response in patients with psoriasis involving at least 3% BSA at baseline).4,5 Rapid separation in ASAS 40 response rates observed within 1–2 weeks after a single dose of BIMZELX vs placebo; 16.4% (21/128) vs 1.6% (2/126) at Week 1 (nominal p<0.001) in BE MOBILE 1, and 16.7% (37/221) vs 7.2% (8/111) at Week 2 (nominal p=0.019) in BE MOBILE 2 (NRI analysis).3,7,8 At Week 2, ASDAS <2.1 achieved by 19.6% (25/128) of BIMZELX-treated patients vs 7.4% (n=9/126) placebo in BE MOBILE 1 and 24.6% (54/221) vs 8.4% (9/111) in BE MOBILE 2, respectively (MI).7,8 ASDAS <2.1 achieved by 61.6% (79/128) nr-axSpA patients and 57.1% (126/221) AS patients at Week 52 in BE MOBILE 1 and BE MOBILE 2 respectively (exploratory endpoint, MI analysis).3,9
▼This medicine is subject to additional monitoring. This will allow quick identification of new safety information. Adverse events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov.uk for the UK and hpra.ie/homepage/about-us/report-an-issue for Republic of Ireland. Adverse events should also be reported to UCB Pharma Ltd at ucbcares.uk@ucb.com or 0800 2793177 for the UK and UCB (Pharma) Ireland Ltd at ucbcares.ie@ucb.com or 1800 930075 for Republic of Ireland.
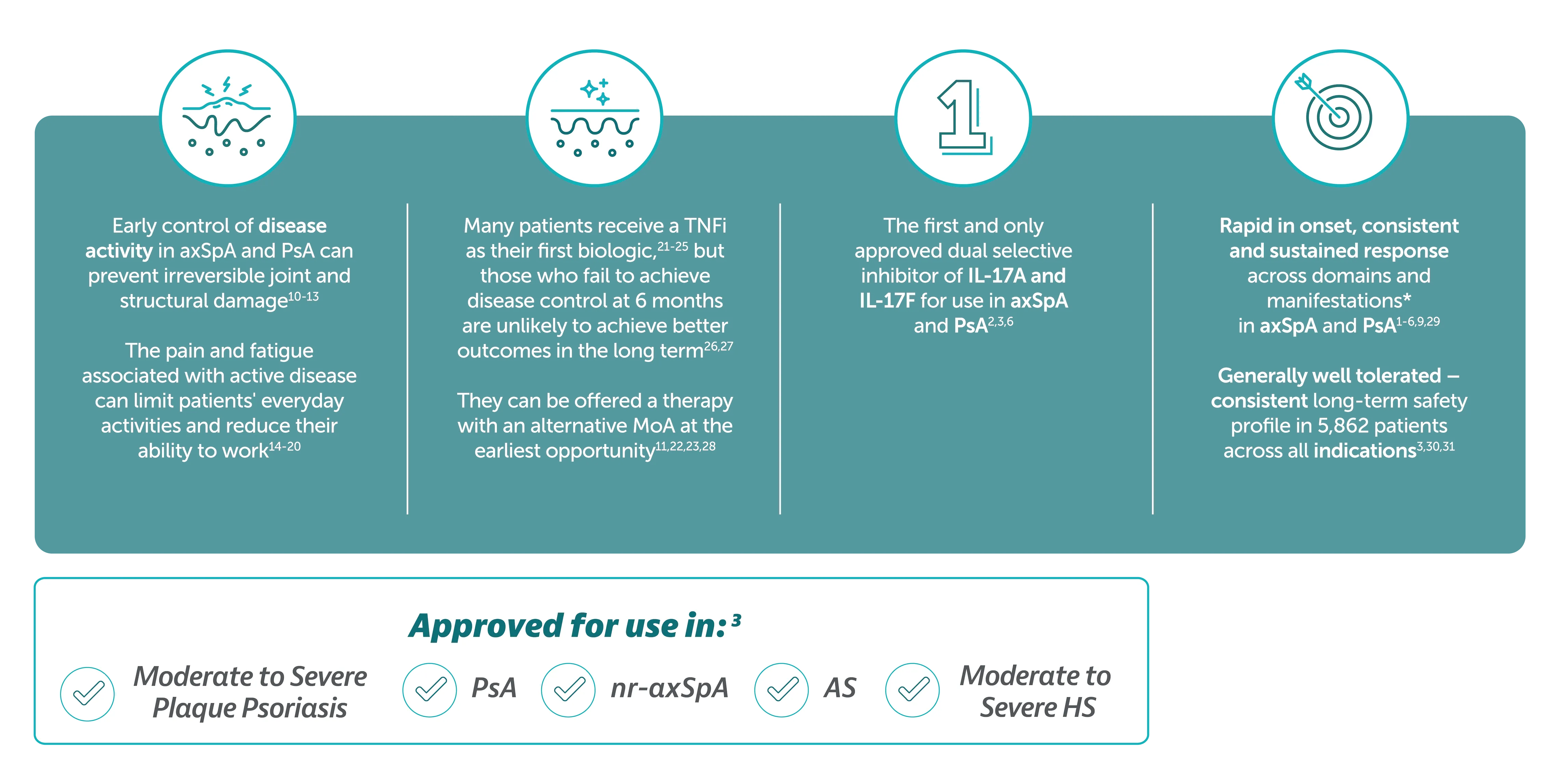
*ACR 50 and PASI 90 for PsA, ASAS 40 and ASDAS <2.1 for axSpA
BIMZELX® (bimekizumab) is indicated for the treatment of: active PsA, alone or in combination with methotrexate, in adults who have had an inadequate response or who have been intolerant to one or more DMARDs; active nr-axSpA, in adults with objective signs of inflammation as indicated by elevated CRP and/or MRI, who have responded inadequately or are intolerant to NSAIDs; and active AS, in adults who have responded inadequately or are intolerant to conventional therapy.3



IE-BK-2400113
Date of creation: October 2025